

Pathogenesis of prediabetes: role of the liver in isolated fasting hyperglycemia and combined fasting and postprandial hyperglycemia
- PMID: 23345093
- PMCID: PMC3590488
- DOI: 10.1210/jc.2012-3056
Pathogenesis of prediabetes: role of the liver in isolated fasting hyperglycemia and combined fasting and postprandial hyperglycemia
Abstract
Context: People with prediabetes are at high risk of developing diabetes.
Objective: The objective of this study was to determine the pathogenesis of fasting and postprandial hyperglycemia in prediabetes.
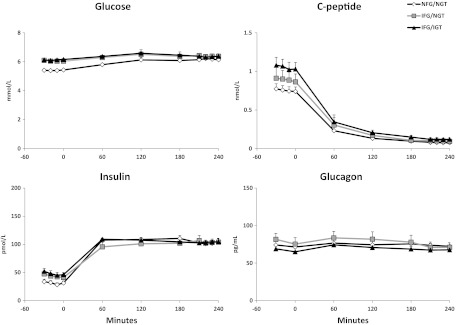
Design: Glucose production, gluconeogenesis, glycogenolysis, and glucose disappearance were measured before and during a hyperinsulinemic clamp using [6,6-(2)H2]glucose and the deuterated water method corrected for transaldolase exchange.
Setting: The study was conducted at the Mayo Clinic Clinical Research Unit.
Participants: Subjects with impaired fasting glucose (IFG)/normal glucose tolerance (NGT) (n = 14), IFG/impaired glucose tolerance (IGT) (n = 18), and normal fasting glucose (NFG)/NGT (n = 16) were studied.
Intervention: A hyperinsulinemic clamp was used.
Outcome measures: Glucose production, glucose disappearance, gluconeogenesis, and glycogenolysis were measured.
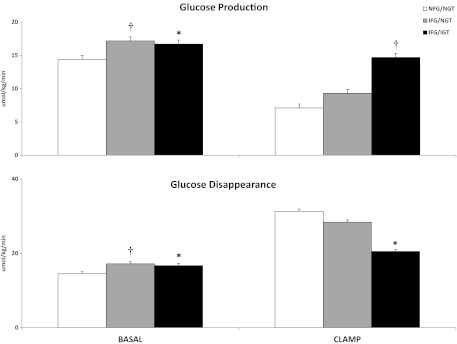
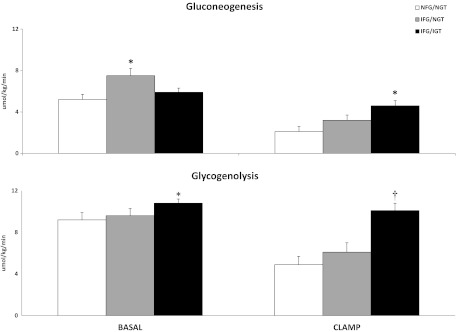
Results: Fasting glucose production was higher (P < .0001) in subjects with IFG/NGT than in those with NFG/NGT because of increased rates of gluconeogenesis (P = .003). On the other hand, insulin-induced suppression of glucose production, gluconeogenesis, glycogenolysis, and stimulation of glucose disappearance all were normal. Although fasting glucose production also was increased (P = .0002) in subjects with IFG/IGT, insulin-induced suppression of glucose production, gluconeogenesis, and glycogenolysis and stimulation of glucose disappearance were impaired (P = .005).
Conclusions: Fasting hyperglycemia is due to excessive glucose production in people with either IFG/NGT or IFG/IGT. Both insulin action and postprandial glucose concentrations are normal in IFG/NGT but abnormal in IFG/IGT. This finding suggests that hepatic and extrahepatic insulin resistance causes or exacerbates postprandial glucose intolerance in IFG/IGT. Elevated gluconeogenesis in the fasting state in IFG/NGT and impaired insulin-induced suppression of both gluconeogenesis and glycogenolysis in IFG/IGT suggest that alteration in the regulation of these pathways occurs early in the evolution of type 2 diabetes.
Figures
References
-
- Dinneen SF, Maldonado D, III, Leibson CL, et al. Effects of changing diagnostic criteria on the risk of developing diabetes. Diabetes Care. 1998;21:1408–1413 - PubMed
-
- Meigs JB, Muller DC, Nathan DM, Blake DR, Andres R. The natural history of progression from normal glucose tolerance to type 2 diabetes in the Baltimore longitudinal study of aging. Diabetes. 2003;52:1475–1484 - PubMed
-
- Saad MF, Knowler WC, Pettitt DJ, Nelson FG, Mott DM, Bennett PH. The natural history of impaired glucose tolerance in the Pima Indians. N Engl J Med. 1988;319:1500–1506 - PubMed
-
- Hanefeld M, Koehler C, Fuecker K, Henkel E, Schaper F, Temelkova-Kurktschiev T. Insulin secretion and insulin sensitivity pattern is different in isolated impaired glucose tolerance and impaired fasting glucose. Diabetes Care. 2003;26:868–874 - PubMed
-
- Bock G, Dalla Man C, Campioni M, et al. Pathogenesis of prediabetes: mechanisms of fasting and postprandial hyperglycemia in people with impaired fasting glucose and/or impaired glucose tolerance. Diabetes. 2006;55:3536–3549 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
