

Risk factors for subtrochanteric and diaphyseal fractures: the study of osteoporotic fractures
- PMID: 23345099
- PMCID: PMC3565107
- DOI: 10.1210/jc.2012-1896
Risk factors for subtrochanteric and diaphyseal fractures: the study of osteoporotic fractures
Abstract
Context: Patients on long-term bisphosphonate therapy may have an increased incidence of low-energy subtrochanteric and diaphyseal (SD) femoral fractures. However, the incidence and risk factors associated with these fractures have not been well defined.
Objective: The objective of the study was to determine the incidence of and risk factors for low-energy SD fractures in the Study of Osteoporotic Fractures (SOF).
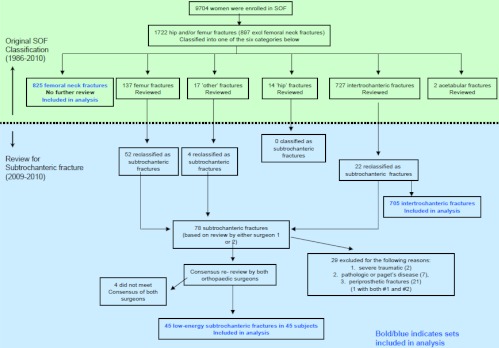
Design: Low-energy SD fractures were identified from a review of radiographic reports obtained between 1986 and 2010 in women in the SOF. Among the SD fractures, pathological, periprosthetic, and traumatic fractures were excluded. We assessed risk factors for SD fractures as well as risk factors for femoral neck (FN) and intertrochanteric (IT) hip fractures using both age-adjusted and multivariate time-dependent proportional hazards models. During this follow-up, only a small minority had ever used bisphosphonates.
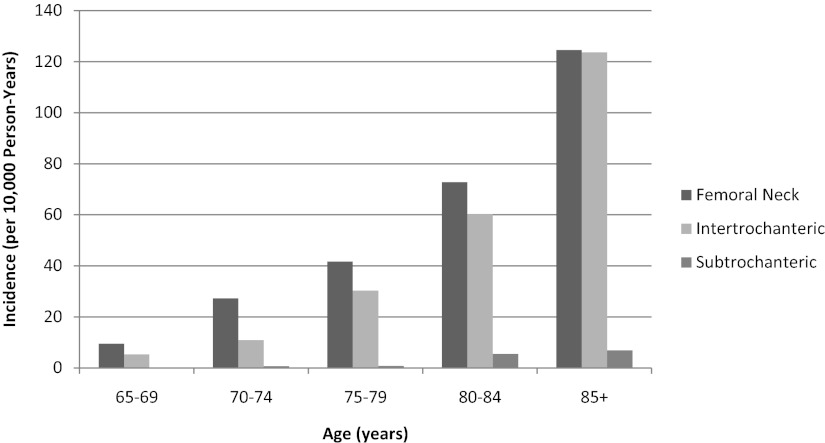
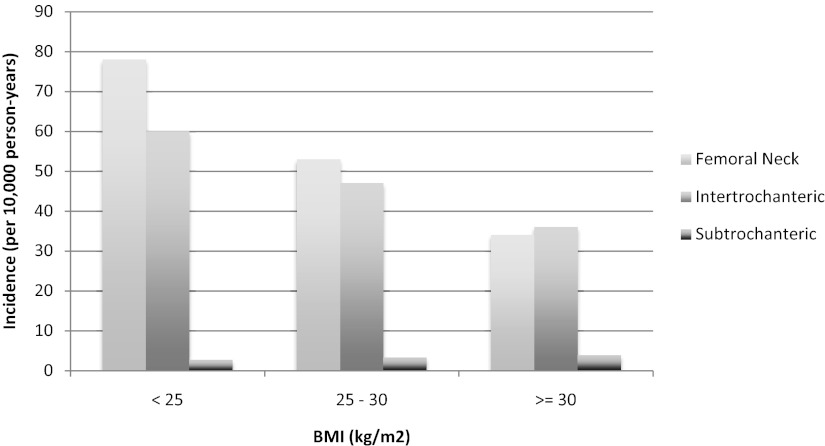
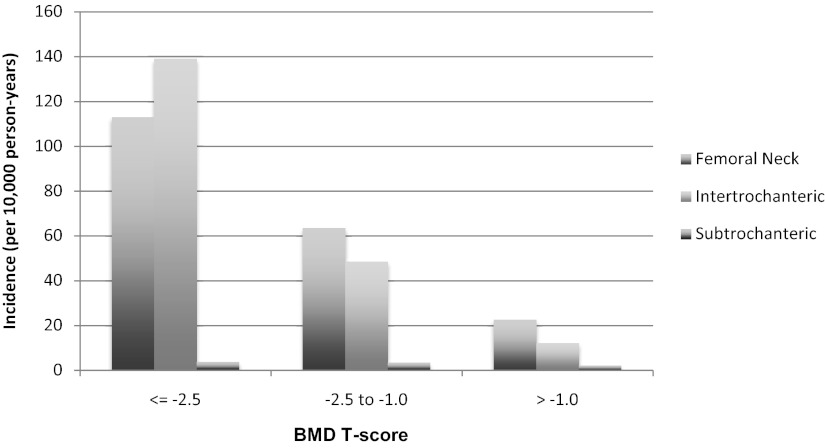
Results: Forty-five women sustained low-energy subtrochanteric/diaphyseal femoral fractures over a total follow-up of 140 000 person-years. The incidence of SD fracture was 3.2 per 10 000 person-years compared with a total hip fracture incidence of 110 per 10 000 person-years. A total of about 12% of women reported bisphosphonate use at 1 or more visits. In multivariate analyses, age, total hip bone mineral density (BMD), bisphosphonate use, and history of diabetes emerged as independent risk factors for SD fractures. Risk factors for FN and IT fractures included age, BMD, and history of falls or prior fractures. Bisphosphonate use was protective against FN fractures, whereas there was an increased risk of SD fractures (hazard ratio 2.58, P = .049) with bisphosphonate use after adjustment for other risk factors for fracture.
Conclusions: In SOF, low-energy SD fractures were rare occurrences, far outnumbered by FN and IT fractures. Typical risk factors were associated with FN and IT fractures, whereas only age, total hip BMD, and history of diabetes were independent risk factors for SD fractures. In addition, bisphosphonate use was a marginally significantly predictor although the SOF study has limited ability to assess this association.
Figures
References
-
- Shane E, Burr D, Ebeling PR, et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010;25:2267–2294 - PubMed
-
- Odvina CV, Levy S, Rao S, Zerwekh JE, Sudhaker Rao D. Unusual mid-shaft fractures during long term bisphosphonate therapy. Clin Endocrinol (Oxf). 2009;72(2):161–168 - PubMed
-
- Armamento-Villareal R, Napoli N, Diemer K, et al. Bone turnover in bone biopsies of patients with low-energy cortical fractures receiving bisphosphonates: a case series. Calcif Tissue Int. 2009;85:37–44 - PubMed
-
- Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate. N Engl J Med. 2008;358:1304–1306 - PubMed
-
- Giusti A, Hamdy NA, Papapoulos SE. Atypical fractures of the femur and bisphosphonate therapy. A systematic review of case/case series studies. Bone. 2010;47:169–180 - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG008415/AG/NIA NIH HHS/United States
- AG05407/AG/NIA NIH HHS/United States
- R01 AR035583/AR/NIAMS NIH HHS/United States
- AR35582/AR/NIAMS NIH HHS/United States
- AG05394/AG/NIA NIH HHS/United States
- AR46238/AR/NIAMS NIH HHS/United States
- AG005394-22A1/AG/NIA NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- AG027576-22/AG/NIA NIH HHS/United States
- AR35583/AR/NIAMS NIH HHS/United States
- AG005407/AG/NIA NIH HHS/United States
- R01 AG030474/AG/NIA NIH HHS/United States
- R01 AR035582/AR/NIAMS NIH HHS/United States
- AR35584/AR/NIAMS NIH HHS/United States
- R01 AG027574/AG/NIA NIH HHS/United States
- R01 AR035584/AR/NIAMS NIH HHS/United States
- AG027574-22A1/AG/NIA NIH HHS/United States
- R01 AG027576/AG/NIA NIH HHS/United States
- AG030474/AG/NIA NIH HHS/United States
- AG08415/AG/NIA NIH HHS/United States
- R01 AR046238/AR/NIAMS NIH HHS/United States
- R01 AG005394/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
