

A Rare Case of Kikuchi Fujimoto's Disease with Subsequent Development of Systemic Lupus Erythematosus
- PMID: 23346446
- PMCID: PMC3546453
- DOI: 10.1155/2012/325062
A Rare Case of Kikuchi Fujimoto's Disease with Subsequent Development of Systemic Lupus Erythematosus
Abstract
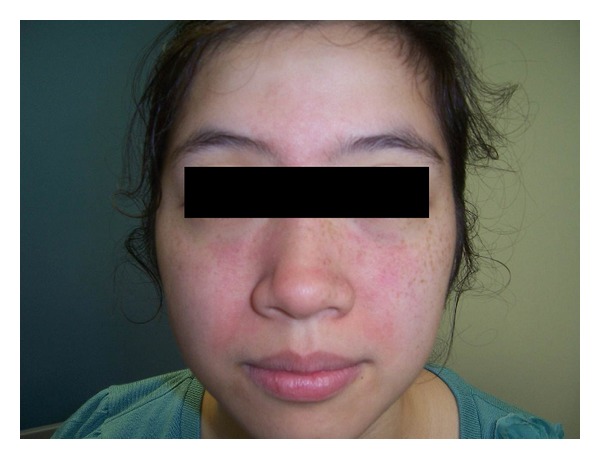
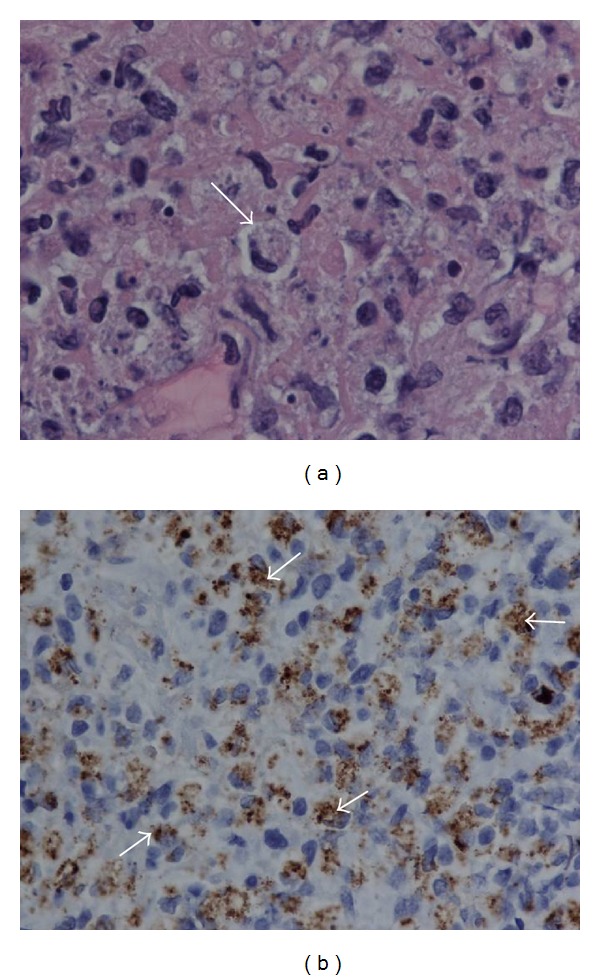
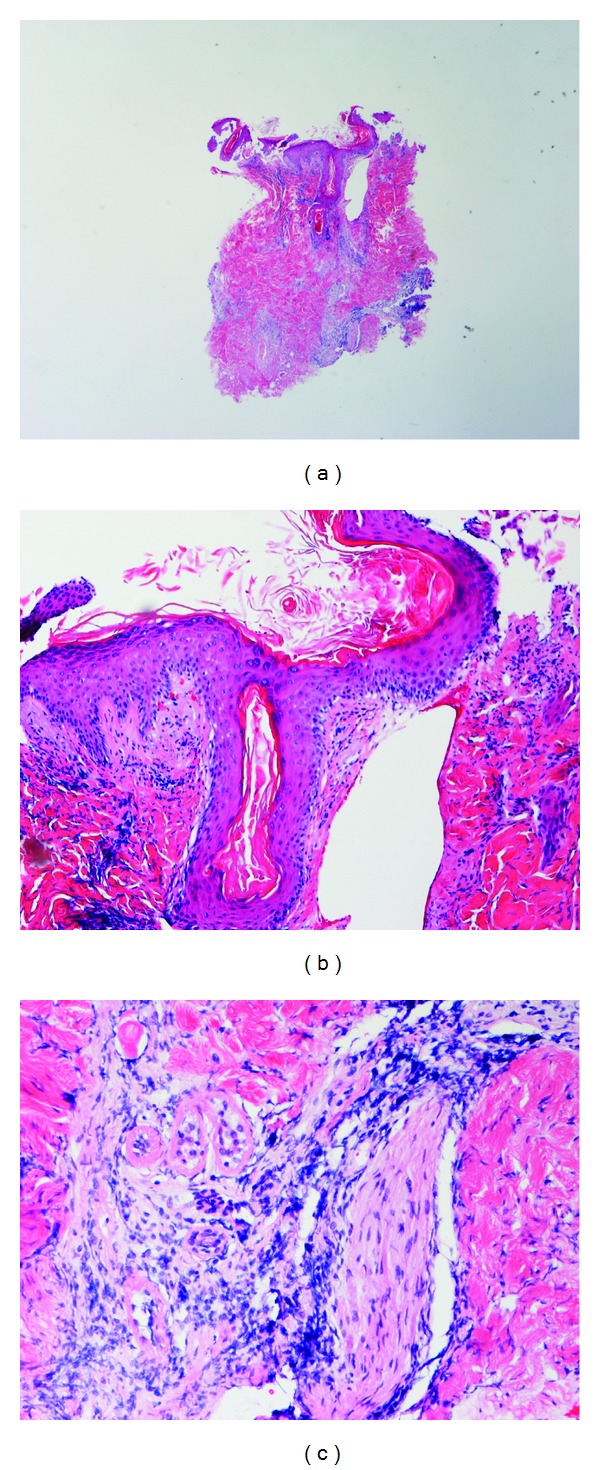
Kikuchi Fujimoto's disease (KFD) is a rare, immune-mediated, self-limiting disorder with unique histopathological features. KFD is usually seen in young Asian females; however, cases have been reported throughout the world and in all ethnicities. It has been recognized that there is a rare association between Systemic Lupus Erythematosus (SLE) and KFD via sporadic case reports. The exact pathophysiological relationship between these two diseases is still unclear. We report a case of a young Asian female who presented with persistent fever and lymphadenopathy and was diagnosed with Kikuchi Fujimoto's disease based on lymph node biopsy; although an SLE workup was done, she did not meet the American Rheumatology Association (ARA) diagnostic criteria for lupus, and the lymph node biopsy did not show features of SLE. She improved clinically with a short course of steroid therapy. Two months later, the patient presented with central facial rash and arthralgia. SLE workup was repeated, a skin biopsy was done, and the results at this time supported a diagnosis of SLE.
Figures

References
-
- Kikuchi M. Lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytes. Acta haematologica Japonica. 1972;35:379–380.
-
- Fujimoto Y, Kojima Y, Yamaguchi K. Cervical Subacute necrotizing lymphadenitits. Naika. 1972;20:920–927.
-
- Kucukardali Y, Solmazgul E, Kunter E, Oncul O, Yildirim S, Kaplan M. Kikuchi-fujimoto disease: analysis of 244 cases. Clinical Rheumatology. 2007;26(1):50–54. - PubMed
-
- Hrycek A, Cieślik P, Szkróbka W, Pajak J. Kikuchi-Fujimoto disease: a case report. RRheumatology International. 2005;26(2):179–181. - PubMed
-
- Bailey EM, Klein NC, Cunha BA. Kikuchi's disease with liver dysfunction presenting as fever of unknown origin. The Lancet. 1989;2(8669):p. 986. - PubMed
LinkOut - more resources
Full Text Sources
