

Two Cases of Laparoscopic Adhesiolysis for Chronic Abdominal Pain without Intestinal Obstruction after Total Gastrectomy
- PMID: 23346498
- PMCID: PMC3543976
- DOI: 10.5230/jgc.2012.12.4.249
Two Cases of Laparoscopic Adhesiolysis for Chronic Abdominal Pain without Intestinal Obstruction after Total Gastrectomy
Abstract
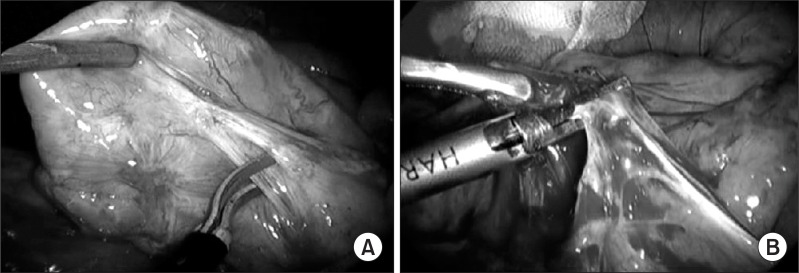
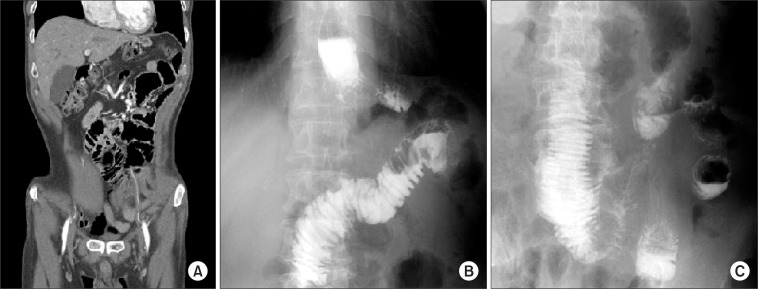
Chronic abdominal pain remains a challenge to all known diagnostic and treatment methods with patients undergoing numerous diagnostic work-ups including surgery. However, the surgical treatment of patients with chronic intractable abdominal pain is controversial. There has been no discussion of the indications for adhesiolysis in cases of obstruction or strangulation of the bowel, and adhesiolysis by laparotomy has never gained acceptance as a treatment modality for chronic abdominal pain. One of the reasons for this lack of acceptance is the high complication rate during and after adhesiolysis. Laparoscopic surgery has been accepted as a technique for diagnostic and therapeutic procedures in general surgery. Laparoscopy allows surgeons to see and treat many abdominal changes that could not otherwise be diagnosed. Here we report two cases of successful symptomatic improvement through laparoscopic adhesiolysis for chronic abdominal pain without intestinal obstruction after total gastrectomy.
Keywords: Abdominal pain; Adhesion; Gastrectomy; Laparoscopy.
Figures

Similar articles
-
The role of laparoscopic adhesiolysis in the treatment of patients with chronic abdominal pain or recurrent bowel obstruction.JSLS. 2002 Apr-Jun;6(2):111-4. JSLS. 2002. PMID: 12113412 Free PMC article.
-
Laparoscopic adhesiolysis for small bowel obstruction.Am J Surg. 2004 Apr;187(4):464-70. doi: 10.1016/j.amjsurg.2003.12.036. Am J Surg. 2004. PMID: 15041492 Review.
-
Laparoscopic adhesiolysis in patients with chronic abdominal pain: a blinded randomised controlled multi-centre trial.Lancet. 2003 Apr 12;361(9365):1247-51. doi: 10.1016/s0140-6736(03)12979-0. Lancet. 2003. PMID: 12699951 Clinical Trial.
-
A prospective analysis of predictive factors on the results of laparoscopic adhesiolysis in patients with chronic abdominal pain.Surg Laparosc Endosc Percutan Tech. 2003 Apr;13(2):88-94. doi: 10.1097/00129689-200304000-00006. Surg Laparosc Endosc Percutan Tech. 2003. PMID: 12709613
-
Laparoscopic adhesiolysis in patients with chronic abdominal pain.Curr Opin Obstet Gynecol. 2004 Aug;16(4):313-8. doi: 10.1097/01.gco.0000136497.02700.e0. Curr Opin Obstet Gynecol. 2004. PMID: 15232485 Review.
Cited by
-
Chronic abdominal syndrome due to nervous compression. Study of 100 cases and proposed diagnostic-therapeutic algorithm.J Gastrointest Surg. 2015 Jun;19(6):1059-71. doi: 10.1007/s11605-015-2801-8. Epub 2015 Mar 24. J Gastrointest Surg. 2015. PMID: 25801595 Free PMC article.
References
-
- Swank DJ, Jeekel H. Laparoscopic adhesiolysis in patients with chronic abdominal pain. Curr Opin Obstet Gynecol. 2004;16:313–318. - PubMed
-
- Swank DJ, van Erp WF, Repelaer van Driel OJ, Hop WC, Bonjer HJ, Jeekel J. Complications and feasibility of laparoscopic adhesiolysis in patients with chronic abdominal pain. A retrospective study. Surg Endosc. 2002;16:1468–1473. - PubMed
-
- Paajanen H, Julkunen K, Waris H. Laparoscopy in chronic abdominal pain: a prospective nonrandomized long-term follow-up study. J Clin Gastroenterol. 2005;39:110–114. - PubMed
-
- Swank DJ, Van Erp WF, Repelaer van Driel OJ, Hop WC, Bonjer HJ, Jeekel H. A prospective analysis of predictive factors on the results of laparoscopic adhesiolysis in patients with chronic abdominal pain. Surg Laparosc Endosc Percutan Tech. 2003;13:88–94. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
