The use of a staged drainage seton for the treatment of anal fistulae or fistulous abscesses
- PMID: 23346510
- PMCID: PMC3548146
- DOI: 10.3393/jksc.2012.28.6.309
The use of a staged drainage seton for the treatment of anal fistulae or fistulous abscesses
Abstract
Purpose: The aim of this retrospective study was to evaluate the rate of recurrence and incontinence after the treatment of fistulae or fistulous abscesses by using the staged drainage seton method.
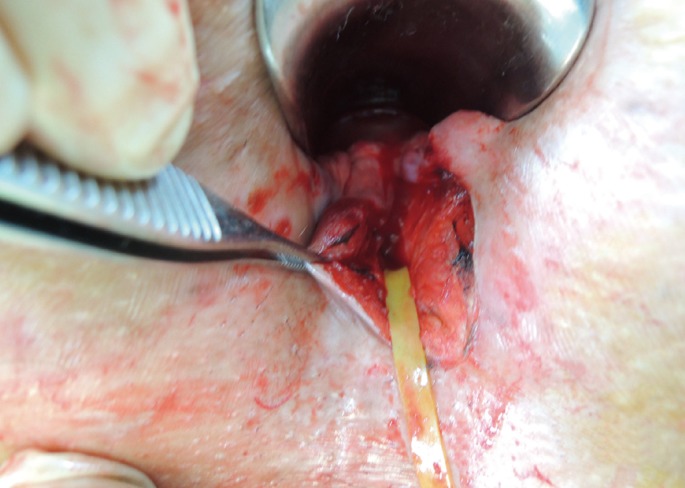
Methods: According to the condition, a drainage seton alone or a drainage seton combined with internal opening (IO) closure and relocation of the seton was used. After a period of time, the seton was changed with 3-0 nylon; then, after another period of time, the authors terminated the treatment by removing the 3-0 nylon. Telephone interviews were used for follow-up. The following were evaluated: the relationship between the type of fistula and recurrence; the relationship between the type of fistula and the period of treatment; the relationship between the recurrence and presence of abscess; the relationship between IO closure and recurrence; the relationship between the period of seton change and recurrence; reported continence for flatus, liquid stool, and solid stool.
Results: The recurrence rate of fistulae or suppuration was 6.5%, but for cases of horseshoe extension, the recurrence rate was 57.1%. The rate of recurrence was related to the type of fistula (P = 0.001). Incontinence developed in 3.8% of the cases. No statistically significant relationship was found between the rate of recurrence and the presence of an abscess or between the closure of the IO and the period of seton change or removal.
Conclusion: In the treatment of anal fistulae or fistulous abscesses, the use of a staged drainage seton can reduce the rate of recurrence and incontinence.
Keywords: Fistula; Perianal abscess; Seton; Surgical drainage.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures






Similar articles
-
Comparison of the Efficacy of the Various Treatment Modalities in the Management of Perianal Crohn's Fistula: A Review.Cureus. 2020 Dec 3;12(12):e11882. doi: 10.7759/cureus.11882. Cureus. 2020. PMID: 33415035 Free PMC article. Review.
-
The use of a loose seton as a definitive surgical treatment for anorectal abscesses and complex anal fistulas.Adv Clin Exp Med. 2023 Oct;32(10):1149-1157. doi: 10.17219/acem/161162. Adv Clin Exp Med. 2023. PMID: 36920266
-
Perianal abscess in Crohn's disease.Dis Colon Rectum. 1997 Apr;40(4):443-50. doi: 10.1007/BF02258390. Dis Colon Rectum. 1997. PMID: 9106694
-
Predictive factors for recurrence of high transsphincteric anal fistula after placement of seton.J Surg Res. 2017 Jun 1;213:261-268. doi: 10.1016/j.jss.2017.02.053. Epub 2017 Mar 6. J Surg Res. 2017. PMID: 28601324
-
A systematic review and meta-analysis of incision and seton drainage in the treatment of high perianal abscess.Ann Palliat Med. 2021 Sep;10(9):9830-9840. doi: 10.21037/apm-21-2229. Ann Palliat Med. 2021. PMID: 34628909
Cited by
-
Management of Fistula-in-Ano-The Current Evidence.Indian J Surg. 2014 Dec;76(6):482-6. doi: 10.1007/s12262-014-1150-2. Epub 2014 Aug 15. Indian J Surg. 2014. PMID: 25614724 Free PMC article.
-
Video-Assisted Anal Fistula Treatment (VAAFT) for Complex Anal Fistula: A Preliminary Evaluation in China.Med Sci Monit. 2017 Apr 30;23:2065-2071. doi: 10.12659/msm.904055. Med Sci Monit. 2017. PMID: 28456815 Free PMC article.
-
Anal Fistula Laser Closure: the length of fistula is the Achilles' heel.Tech Coloproctol. 2018 Dec;22(12):933-939. doi: 10.1007/s10151-018-1885-z. Epub 2018 Dec 8. Tech Coloproctol. 2018. PMID: 30535666
-
The role of loose seton in the management of anal fistula: a multicenter study of 200 patients.Tech Coloproctol. 2014 Oct;18(10):915-9. doi: 10.1007/s10151-014-1186-0. Epub 2014 Jul 3. Tech Coloproctol. 2014. PMID: 24989839
-
Comparison of the Efficacy of the Various Treatment Modalities in the Management of Perianal Crohn's Fistula: A Review.Cureus. 2020 Dec 3;12(12):e11882. doi: 10.7759/cureus.11882. Cureus. 2020. PMID: 33415035 Free PMC article. Review.
References
-
- Kennedy HL, Zegarra JP. Fistulotomy without external sphincter division for high anal fistulae. Br J Surg. 1990;77:898–901. - PubMed
-
- Jones IT, Fazio VW, Jagelman DG. The use of transanal rectal advancement flaps in the management of fistulas involving the anorectum. Dis Colon Rectum. 1987;30:919–923. - PubMed
-
- Wedell J, Meier zu Eissen P, Banzhaf G, Kleine L. Sliding flap advancement for the treatment of high level fistulae. Br J Surg. 1987;74:390–391. - PubMed
-
- Reznick RK, Bailey HR. Closure of the internal opening for treatment of complex fistula-in-ano. Dis Colon Rectum. 1988;31:116–118. - PubMed
-
- Athanasiadis S, Helmes C, Yazigi R, Kohler A. The direct closure of the internal fistula opening without advancement flap for transsphincteric fistulas-in-ano. Dis Colon Rectum. 2004;47:1174–1180. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources