

Resource use trajectories for aged medicare beneficiaries with complex coronary conditions
- PMID: 23347002
- PMCID: PMC3625399
- DOI: 10.1111/1475-6773.12028
Resource use trajectories for aged medicare beneficiaries with complex coronary conditions
Abstract
Objective: To use coronary revascularization choice to illustrate the application of a method simulating a treatment's effect on subsequent resource use.
Data sources: Medicare inpatient and outpatient claims from 2002 to 2008 for patients receiving multivessel revascularization for symptomatic coronary disease in 2003-2004.
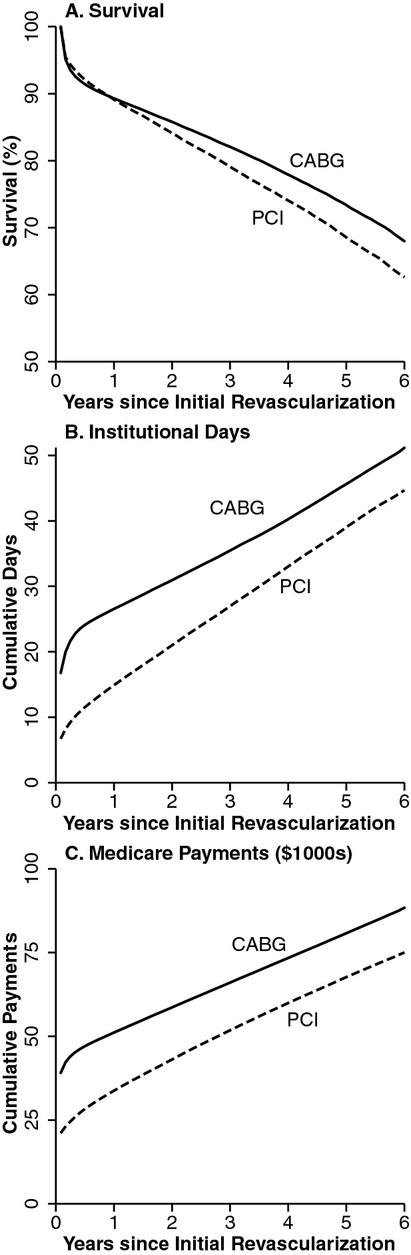
Study design: This retrospective cohort study of 102,877 beneficiaries assessed survival, days in institutional settings, and Medicare payments for up to 6 years following receipt of percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG).
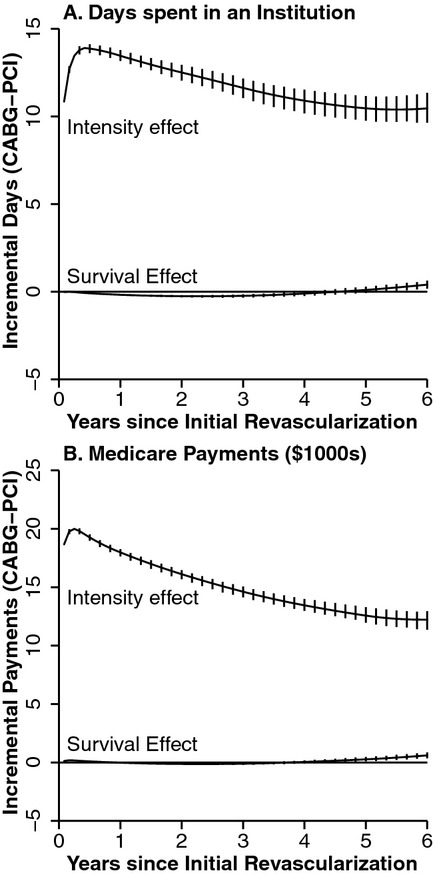
Methods: A three-part estimator designed to provide robust estimates of a treatment's effect in the setting of mortality and censored follow-up was used. The estimator decomposes the treatment effect into effects attributable to survival differences versus treatment-related intensity of resource use.
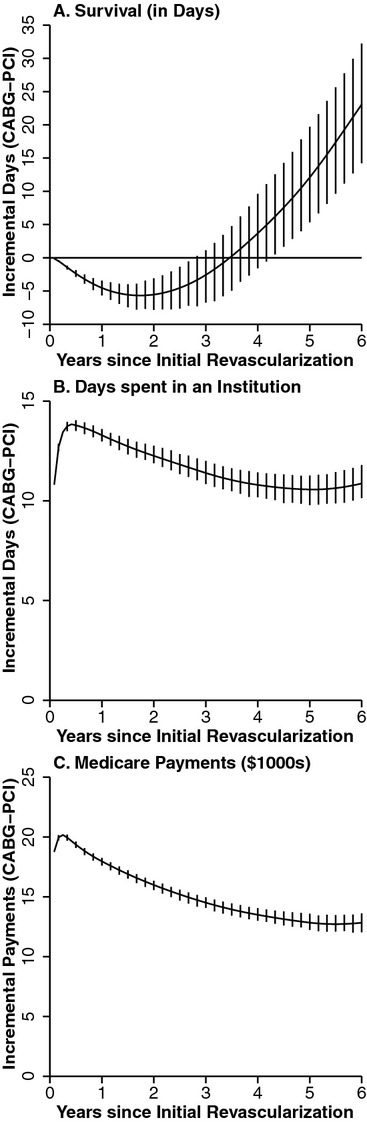
Principal findings: After adjustment, on average CABG recipients survived 23 days longer, spent an 11 additional days in institutional settings, and had cumulative Medicare payments that were $12,834 higher than PCI recipients. The majority of the differences in institutional days and payments were due to intensity rather than survival effects.
Conclusions: In this example, the survival benefit from CABG was modest and the resource implications were substantial, although further adjustments for treatment selection are needed.
© Health Research and Educational Trust.
Figures
Similar articles
-
Impact of Medicare's Bundled Payments Initiative on Patient Selection, Payments, and Outcomes for Percutaneous Coronary Intervention and Coronary Artery Bypass Grafting.Circ Cardiovasc Qual Outcomes. 2020 Sep;13(9):e006171. doi: 10.1161/CIRCOUTCOMES.119.006171. Epub 2020 Sep 1. Circ Cardiovasc Qual Outcomes. 2020. PMID: 32867514 Free PMC article.
-
Association of coronary CT angiography or stress testing with subsequent utilization and spending among Medicare beneficiaries.JAMA. 2011 Nov 16;306(19):2128-36. doi: 10.1001/jama.2011.1652. JAMA. 2011. PMID: 22089720
-
Comparison of multiple drug-eluting stent percutaneous coronary intervention and surgical revascularization in patients with multivessel coronary artery disease: one-year clinical results and total treatment costs.J Invasive Cardiol. 2007 Nov;19(11):469-75. J Invasive Cardiol. 2007. PMID: 17986722 Clinical Trial.
-
Comparing cost aspects of coronary artery bypass graft surgery with coronary artery stenting.J Cardiovasc Surg (Torino). 2012 Oct;53(5):641-50. Epub 2012 Jan 17. J Cardiovasc Surg (Torino). 2012. PMID: 22252542 Review.
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
Cited by
-
Statewide Longitudinal Hospital Use and Charges for Pediatric and Adolescent Patients With Cancer.J Oncol Pract. 2015 Jul;11(4):e468-75. doi: 10.1200/JOP.2014.003590. Epub 2015 Jun 23. J Oncol Pract. 2015. PMID: 26105667 Free PMC article.
-
Age, morbidity, or something else? A residual approach using microdata to measure the impact of technological progress on health care expenditure.Health Econ. 2022 Jun;31(6):1184-1201. doi: 10.1002/hec.4500. Epub 2022 Mar 31. Health Econ. 2022. PMID: 35362244 Free PMC article.
References
-
- Bang H, Tsiatis AS. “Estimating Medical Costs with Censored Data”. Biometrika. 2000;87(2):329–43.
-
- Basu A, Manning WG. “Estimating Lifetime or Episode of Illness Costs under Censoring”. Health Economics. 2010;19(9):1010–28. - PubMed
-
- Bravata DM, Gienger AL, McDonald KM, Sundaram V, Perez MV, Varghese R, Kapoor JR, Ardehali R, Owens DK, Hlatky MA. “Systematic Review: The Comparative Effectiveness of Percutaneous Coronary Interventions and Coronary Artery Bypass Graft Surgery”. Annals of Internal Medicine. 2007;147(10):703. - PubMed
-
- Brennan JM, Peterson ED, Messenger JC, Rumsfeld JS, Weintraub WS, Anstrom KJ, Eisenstein EL, Milford-Beland S, Grau-Sepulveda MV, Booth ME, Dokholyan RS, Douglas PS, Duke DT, Clinical Research Institute “Linking the National Cardiovascular Data Registry CathPCI Registry with Medicare Claims Data: Validation of a Longitudinal Cohort of Elderly Patients Undergoing Cardiac Catheterization”. Circulation: Cardiovascular Quality and Outcomes. 2012;5(1):134–40. - PubMed
-
- Elixhauser A, Steiner C, Harris DR, Coffey RM. “Comorbidity Measures for Use with Administrative Data”. Medical Care. 1998;36(1):8–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
