Provider compliance with guidelines for management of cardiovascular risk in HIV-infected patients
- PMID: 23347705
- PMCID: PMC3557014
- DOI: 10.5888/pcd10.120083
Provider compliance with guidelines for management of cardiovascular risk in HIV-infected patients
Abstract
Introduction: Compliance with National Cholesterol Education Program Adult Treatment Panel III (NCEP) guidelines has been shown to significantly reduce incident cardiovascular events. We investigated physicians' compliance with NCEP guidelines to reduce cardiovascular disease (CVD) risk in a population infected with HIV.
Methods: We analyzed HIV Outpatient Study (HOPS) data, following eligible patients from January 1, 2002, or first HOPS visit thereafter to calculate 10-year cardiovascular risk (10yCVR), until September 30, 2009, death, or last office visit. We categorized participants into four 10yCVR strata, according to guidelines determined by NCEP, the Infectious Disease Society of America, and the Adult AIDS Clinical Trials Group. We calculated percentages of patients treated for dyslipidemia and hypertension, calculated percentages of patients who achieved recommended goals, and categorized them by 10yCVR stratum.
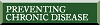
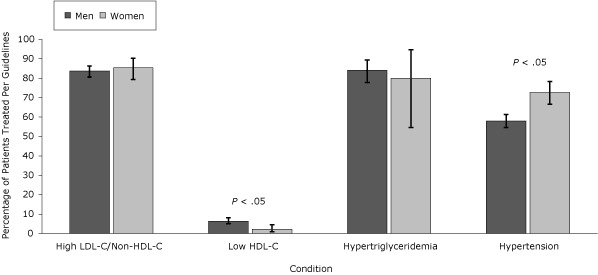
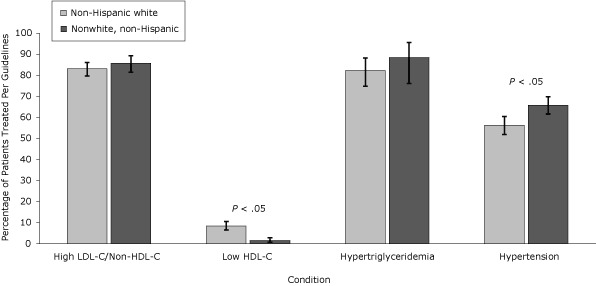
Results: Of 2,005 patients analyzed, 33.7% had fewer than 2 CVD risk factors. For patients who had 2 or more risk factors, 10yCVR was less than 10% for 28.2%, 10% to 20% for 18.2%, and higher than 20% for 20.0% of patients. Of patients eligible for treatment, 81% to 87% were treated for elevated low-density lipoprotein cholesterol/non-high-density lipoprotein cholesterol (LDL-C/non-HDL-C), 2% to 11% were treated for low HDL-C, 56% to 91% were treated for high triglycerides, and 46% to 69% were treated for hypertension. Patients in higher 10yCVR categories were less likely to meet treatment goals than patients in lower 10yCVR categories.
Conclusion: At least one-fifth of contemporary HOPS patients have a 10yCVR higher than 20%, yet a large percentage of at-risk patients who were eligible for pharmacologic treatment did not receive recommended interventions and did not reach recommended treatment goals. Opportunities exist for CVD prevention in the HIV-infected population.
Figures
References
-
- Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004;350(15):1495-504. Erratum in: N Engl J Med 2006;354(7):778. - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285(19):2486–97. 10.1001/jama.285.19.2486 - DOI - PubMed
-
- Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial [summary for patients in Curr Cardiol Rep 2002;4(6):486-7]. Lancet 2002;360(9326):7–22. 10.1016/S0140-6736(02)09327-3 - DOI - PubMed
-
- Sever PS, Dahlöf B, Poulter NR, Wedel H, Beevers G, Caulfield M, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial–Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 2003;361(9364):1149–58. 10.1016/S0140-6736(03)12948-0 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical