

Diagnosis of ocular surface lesions using ultra-high-resolution optical coherence tomography
- PMID: 23347984
- PMCID: PMC3638067
- DOI: 10.1016/j.ophtha.2012.10.025
Diagnosis of ocular surface lesions using ultra-high-resolution optical coherence tomography
Abstract
Purpose: To assess the use of ultra-high-resolution (UHR) optical coherence tomography (OCT) in the diagnosis of ocular surface lesions.
Design: Prospective, noncomparative, interventional case series.
Participants: Fifty-four eyes of 53 consecutive patients with biopsy-proven ocular surface lesions: 8 primary acquired melanosis lesions, 5 amelanotic melanoma lesions, 2 nevi, 19 ocular surface squamous neoplasia lesions, 1 histiocytosis lesion, 6 conjunctival lymphoma lesions, 2 conjunctival amyloidosis lesions, and 11 pterygia lesions.
Intervention: Ultra-high-resolution OCT imaging of the ocular surface lesions.
Main outcome measures: Clinical course and photographs, UHR OCT image, and histopathologic findings.
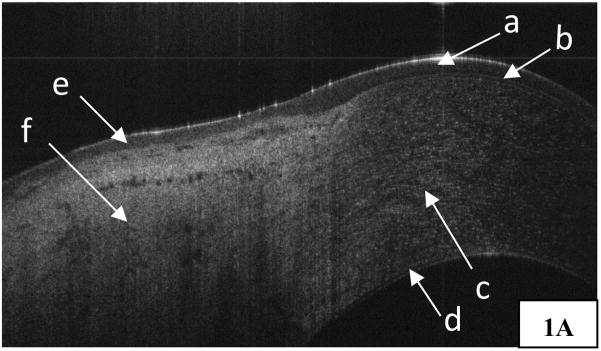
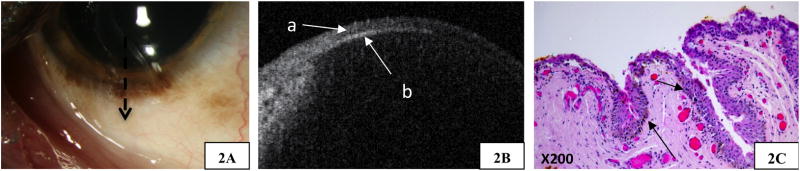
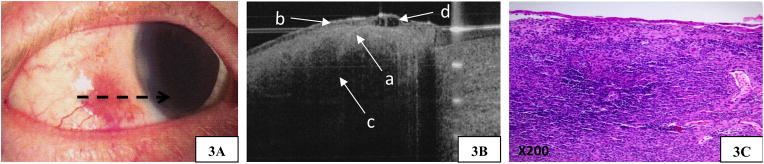
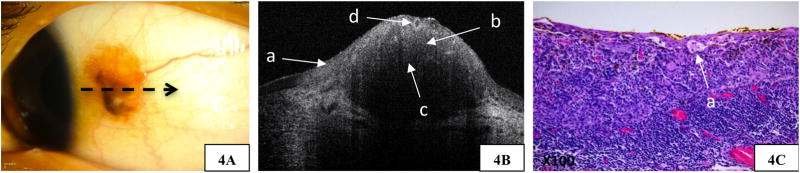
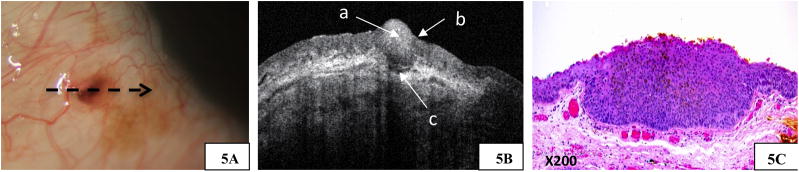
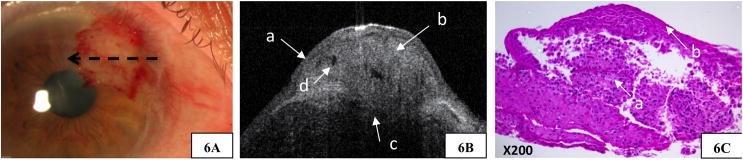
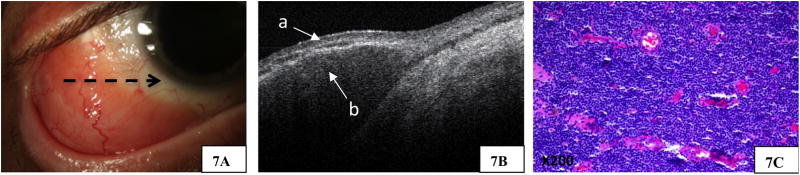
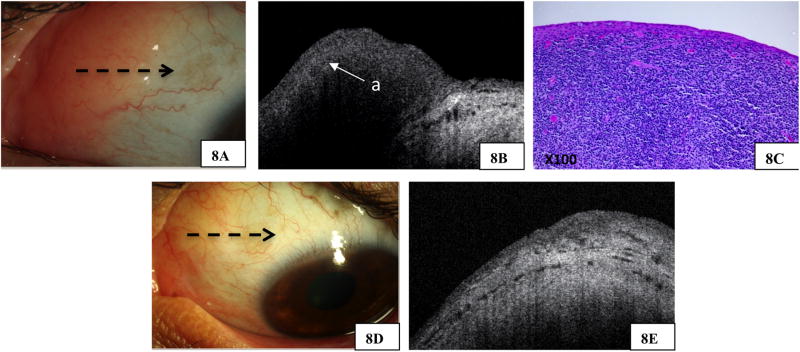
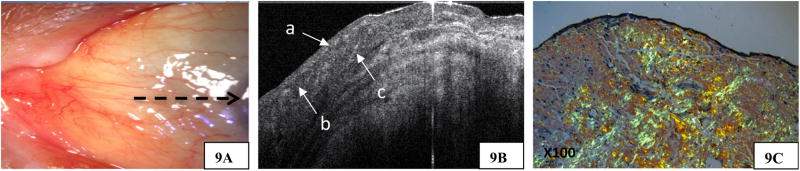
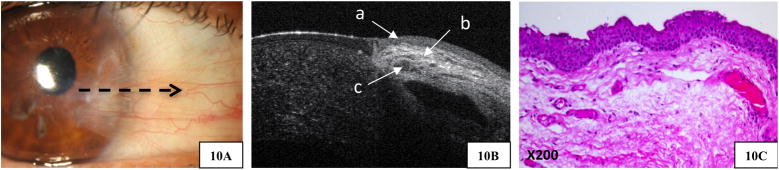
Results: Ultra-high-resolution OCT images of all examined ocular surface lesions showed close correlation with the obtained histopathologic specimens. When clinical differential diagnosis of ocular surface lesions was broad, UHR OCT images provided optical signs indicating a more specific diagnosis and management. In cases of amelanotic melanoma, conjunctival amyloidosis, and primary histiocytosis and in 1 case of ocular surface squamous neoplasia, UHR OCT was instrumental in guiding the diagnosis. In those cases, UHR OCT suggested that the presumed clinical diagnosis was incorrect and favored a diagnosis that later was confirmed by histopathologic examination.
Conclusions: Correlations between UHR OCT and histopathologic findings confirm that UHR OCT is an adjunctive diagnostic method that can provide a noninvasive means to help guide diagnosis and management of ocular surface lesions.
Financial disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussed in this article.
Copyright © 2013 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Diagnosis and management of conjunctival and corneal intraepithelial neoplasia using ultra high-resolution optical coherence tomography.Ophthalmology. 2011 Aug;118(8):1531-7. doi: 10.1016/j.ophtha.2011.01.005. Epub 2011 Apr 20. Ophthalmology. 2011. PMID: 21507486
-
Ultra-high resolution optical coherence tomography for differentiation of ocular surface squamous neoplasia and pterygia.Ophthalmology. 2012 Mar;119(3):481-6. doi: 10.1016/j.ophtha.2011.08.028. Epub 2011 Dec 9. Ophthalmology. 2012. PMID: 22154538
-
Ultra high-resolution anterior segment optical coherence tomography in the diagnosis and management of ocular surface squamous neoplasia.Ocul Surf. 2014 Jan;12(1):46-58. doi: 10.1016/j.jtos.2013.11.001. Epub 2013 Nov 9. Ocul Surf. 2014. PMID: 24439046 Free PMC article. Review.
-
Anterior Segment Swept-Source Optical Coherence Tomography in Ocular Surface Tumors and Simulating Lesions and Correlation With Histopathologic Diagnosis.Cornea. 2025 Mar 28;44(7):806-818. doi: 10.1097/ICO.0000000000003856. Cornea. 2025. PMID: 40152549
-
High-Resolution Optical Coherence Tomography as an Adjunctive Tool in the Diagnosis of Corneal and Conjunctival Pathology.Ocul Surf. 2015 Jul;13(3):226-35. doi: 10.1016/j.jtos.2015.02.001. Epub 2015 Apr 6. Ocul Surf. 2015. PMID: 26045235 Free PMC article. Review.
Cited by
-
Clinical Applications of Anterior Segment Optical Coherence Tomography: An Updated Review.Diagnostics (Basel). 2024 Jan 5;14(2):122. doi: 10.3390/diagnostics14020122. Diagnostics (Basel). 2024. PMID: 38248000 Free PMC article. Review.
-
Applications of Anterior Segment Optical Coherence Tomography in Cornea and Ocular Surface Diseases.J Ophthalmol. 2016;2016:4971572. doi: 10.1155/2016/4971572. Epub 2016 Sep 19. J Ophthalmol. 2016. PMID: 27721988 Free PMC article. Review.
-
AS-OCT Guided Treatment Of Diffuse Conjunctival Squamous Cell Carcinoma With Resection, Amniotic Membrane Graft And Topical Mitomycin C.Clin Ophthalmol. 2019 Nov 20;13:2269-2278. doi: 10.2147/OPTH.S229399. eCollection 2019. Clin Ophthalmol. 2019. PMID: 31819351 Free PMC article.
-
Automatic Segmentation of Corneal Microlayers on Optical Coherence Tomography Images.Transl Vis Sci Technol. 2019 Jun 11;8(3):39. doi: 10.1167/tvst.8.3.39. eCollection 2019 May. Transl Vis Sci Technol. 2019. PMID: 31211004 Free PMC article.
-
Optical coherence tomography imaging of ocular and periocular tumours.Br J Ophthalmol. 2014 Jul;98 Suppl 2(Suppl 2):ii40-6. doi: 10.1136/bjophthalmol-2013-304299. Epub 2014 Mar 5. Br J Ophthalmol. 2014. PMID: 24599420 Free PMC article. Review.
References
-
- Ditta LC, Shildkrot Y, Wilson MW. Outcomes in 15 patients with conjunctival melanoma treated with adjuvant topical mitomycin C: complications and recurrences. Ophthalmology. 2011;118:1754–9. - PubMed
-
- Rudkin AK, Dodd T, Muecke JS. The differential diagnosis of localised amelanotic limbal lesions: a review of 162 consecutive excisions. Br J Ophthalmol. 2011;95:350–4. - PubMed
-
- Meallet MA, Espana EM, Grueterich M, et al. Amniotic membrane transplantation with conjunctival limbal autograft for total limbal stem cell deficiency. Ophthalmology. 2003;110:1585–92. - PubMed
-
- Mathew A, Stumpf T, McGhee C. Impression cytology: implications for ocular surface squamous neoplasia [letter] Br J Ophthalmol. 2008;92:157–8. - PubMed
-
- Balestrazzi A, Martone G, Pichierri P, et al. Corneal invasion of ocular surface squamous neoplasia after clear corneal phacoemulsification: in vivo confocal microscopy analysis. J Cataract Refract Surg. 2008;34:1038–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
