

Is there a role for cyclophilin inhibitors in the management of primary biliary cirrhosis?
- PMID: 23348060
- PMCID: PMC3640509
- DOI: 10.3390/v5020423
Is there a role for cyclophilin inhibitors in the management of primary biliary cirrhosis?
Abstract
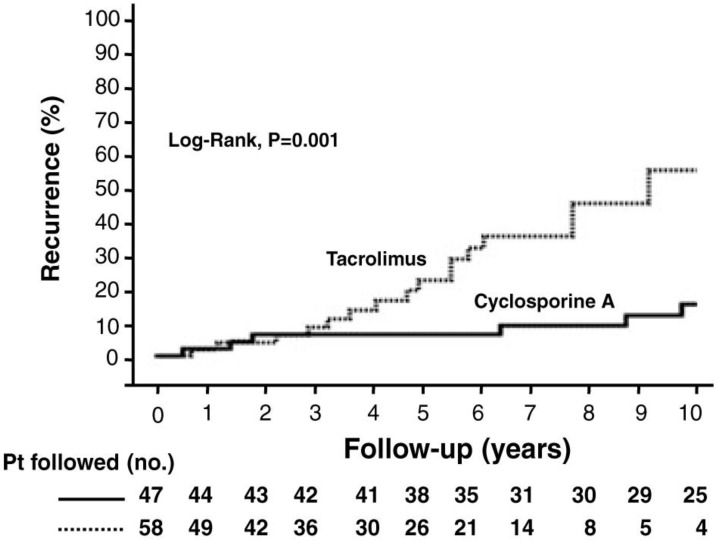
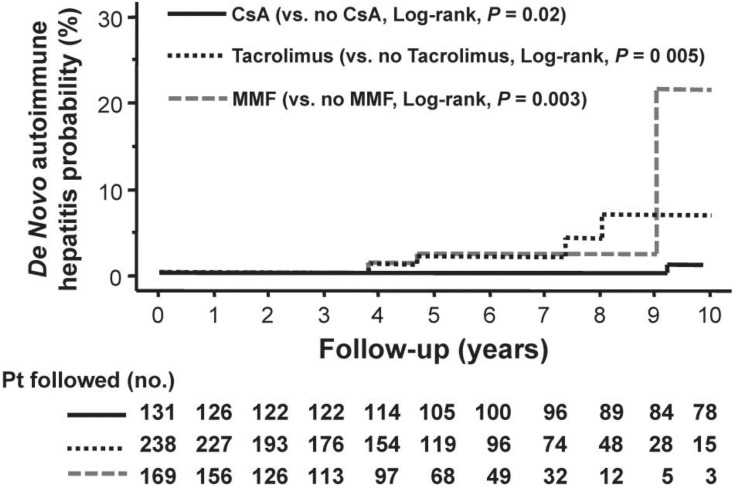
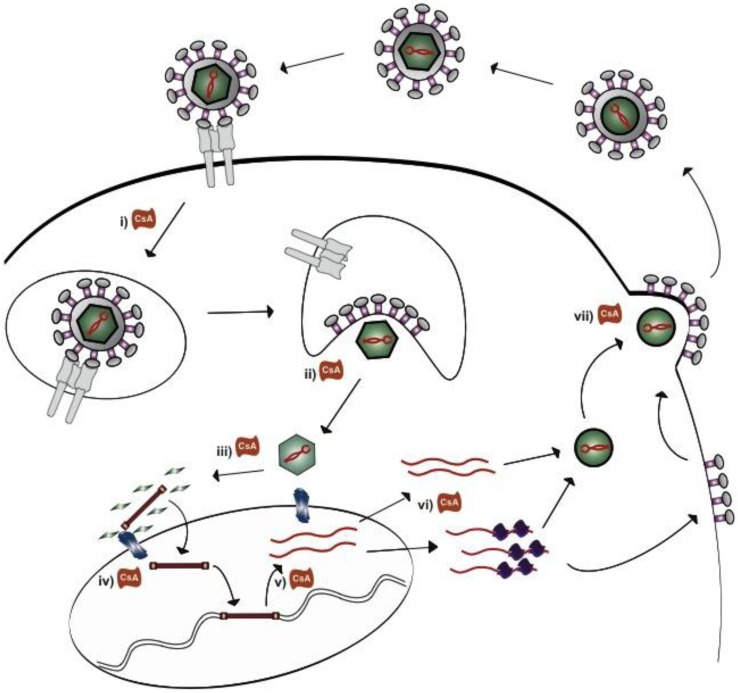
Autoimmune hepatitis (AIH) and primary biliary cirrhosis (PBC) are poorly understood autoimmune liver diseases. Immunosuppression is used to treat AIH and ursodeoxycholic acid is used to slow the progression of PBC. Nevertheless, a proportion of patients with both disorders progress to liver failure. Following liver transplantation, up to a third of patients with PBC experience recurrent disease. Moreover a syndrome referred to as "de novo AIH" occurs in a proportion of patients regardless of maintenance immunosuppression, who have been transplanted for disorders unrelated to AIH. Of note, the use of cyclosporine A appears to protect against the development of recurrent PBC and de novo AIH even though it is a less potent immunosuppressive compared to tacrolimus. The reason why cyclosporine A is protective has not been determined. However, a virus resembling mouse mammary tumor virus (MMTV) has been characterized in patients with PBC and AIH. Accordingly, we hypothesized that the protective effect of cyclosporine A in liver transplant recipients may be mediated by the antiviral activity of this cyclophilin inhibitor. Treatment of the MMTV producing MM5MT cells with different antivirals and immunosuppressive agents showed that both cyclosporine A and the analogue NIM811 inhibited MMTV production from the producer cells. Herein, we discuss the evidence supporting the role of MMTV-like human betaretrovirus in the development of PBC and de novo AIH and speculate on the possibility that the agent may be associated with disease following transplantation. We also review the mechanisms of how both cyclosporine A and NIM811 may inhibit betaretrovirus production in vitro.
Figures
Similar articles
-
Cyclosporine A inhibits in vitro replication of betaretrovirus associated with primary biliary cirrhosis.Liver Int. 2010 Jul;30(6):871-7. doi: 10.1111/j.1478-3231.2010.02257.x. Epub 2010 May 14. Liver Int. 2010. PMID: 20492501
-
Autoimmune hepatitis-primary biliary cirrhosis concurrent with biliary stricture after liver transplantation.World J Gastroenterol. 2015 Feb 21;21(7):2236-41. doi: 10.3748/wjg.v21.i7.2236. World J Gastroenterol. 2015. PMID: 25717264 Free PMC article.
-
Post-liver transplantation de novo hepatitis with overlap features.Pathol Int. 2005 Oct;55(10):660-4. doi: 10.1111/j.1440-1827.2005.01886.x. Pathol Int. 2005. PMID: 16185298
-
[Autoimmune liver diseases and their overlap syndromes].Praxis (Bern 1994). 2006 Sep 6;95(36):1363-81. doi: 10.1024/1661-8157.95.36.1363. Praxis (Bern 1994). 2006. PMID: 16989180 Review. German.
-
Overlap syndromes.Semin Liver Dis. 2005 Aug;25(3):311-20. doi: 10.1055/s-2005-916322. Semin Liver Dis. 2005. PMID: 16143946 Review.
Cited by
-
Linking Human Betaretrovirus with Autoimmunity and Liver Disease in Patients with Primary Biliary Cholangitis.Viruses. 2022 Aug 31;14(9):1941. doi: 10.3390/v14091941. Viruses. 2022. PMID: 36146750 Free PMC article. Review.
-
Searching for Common Mammalian Retroviruses in Pediatric Idiopathic Diseases.Viruses. 2016 Mar 21;8(3):86. doi: 10.3390/v8030086. Viruses. 2016. PMID: 27102168 Free PMC article.
-
Role of novel retroviruses in chronic liver disease: assessing the link of human betaretrovirus with primary biliary cirrhosis.Curr Infect Dis Rep. 2015 Feb;17(2):460. doi: 10.1007/s11908-014-0460-7. Curr Infect Dis Rep. 2015. PMID: 25754451 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
