

Dorsal thoracic arachnoid web and the "scalpel sign": a distinct clinical-radiologic entity
- PMID: 23348759
- PMCID: PMC7964642
- DOI: 10.3174/ajnr.A3432
Dorsal thoracic arachnoid web and the "scalpel sign": a distinct clinical-radiologic entity
Abstract
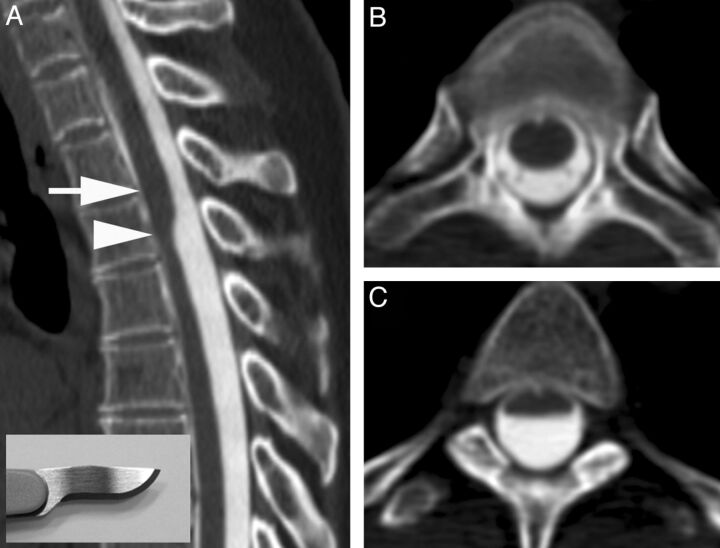
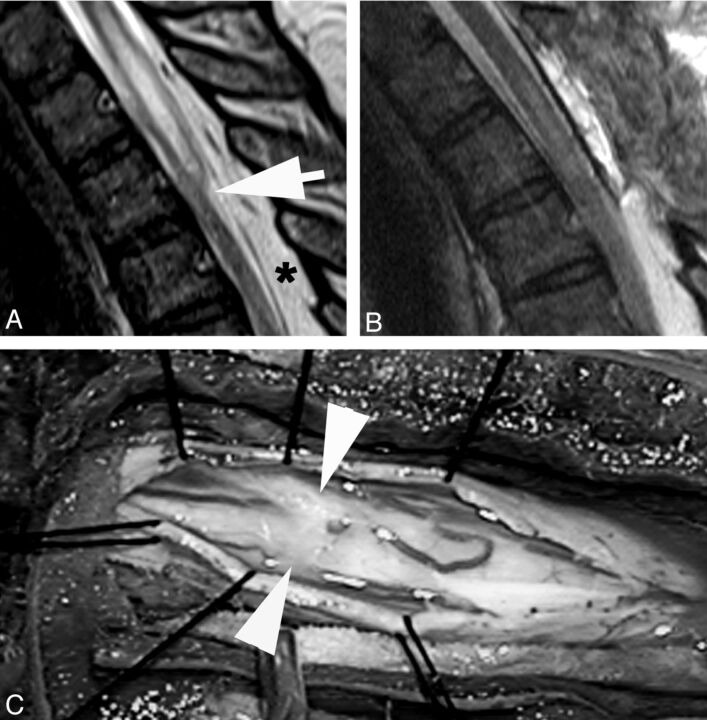
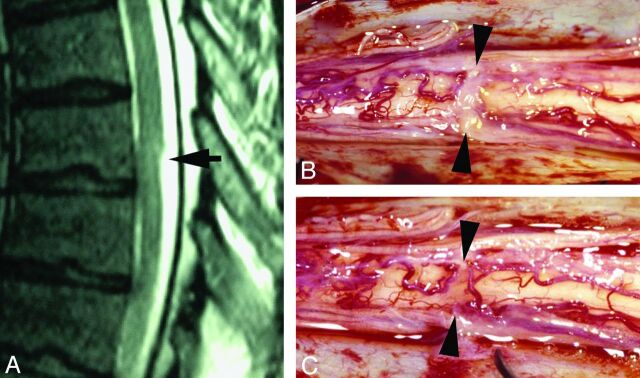
Arachnoid webs are intradural extramedullary bands of arachnoid tissue that can extend to the pial surface of the spinal cord, causing a focal dorsal indentation of the cord. These webs tend to occur in the upper thoracic spine and may produce a characteristic deformity of the cord that we term the "scalpel sign." We describe 14 patients whose imaging studies demonstrated the scalpel sign. Ten of 13 patients who underwent MR imaging demonstrated T2WI cord signal-intensity changes, and 7 of these patients also demonstrated syringomyelia adjacent to the level of indentation. Seven patients underwent surgery, with 5 demonstrating an arachnoid web as the cause of the dorsal indentation demonstrated on preoperative imaging. Although the webs themselves are rarely demonstrated on imaging, we propose that the scalpel sign is a reliable indicator of their presence and should prompt consideration of surgical lysis, which is potentially curative.
Figures



References
-
- Sridharan A, Heilman CB. Transverse dorsal arachnoid web and syringomyelia: case report. Neurosurgery 2009;65:E216–17 - PubMed
-
- Brodbelt AR, Stoodley MA. Syringomyelia and the arachnoid web. Acta Neurochir (Wien) 2003;145:707–11, discussion 711 - PubMed
-
- Paramore CG. Dorsal arachnoid web with spinal cord compression: variant of an arachnoid cyst? Report of two cases. J Neurosurg 2000;93:287–90 - PubMed
-
- Perret G, Green D, Keller J. Diagnosis and treatment of intradural arachnoid cysts of the thoracic spine. Radiology 1962;79:425–29 - PubMed
-
- Holly LT, Batzdorf U. Syringomyelia associated with intradural arachnoid cysts. J Neurosurg Spine 2006;5:111–16 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical