

Correlates of parathyroid hormone concentration in hemodialysis patients
- PMID: 23348879
- PMCID: PMC3685307
- DOI: 10.1093/ndt/gfs598
Correlates of parathyroid hormone concentration in hemodialysis patients
Abstract
Background: The implications of chemical hyperparathyroidism on bone and mineral metabolism measures in maintenance hemodialysis (MHD) are not well known. We hypothesized that a higher serum intact parathyroid hormone (iPTH) level is associated with the higher likelihood of hyperphosphatemia, hyperphosphatasemia [high serum alkaline phosphatase (ALP) levels] and hypercalcemia.
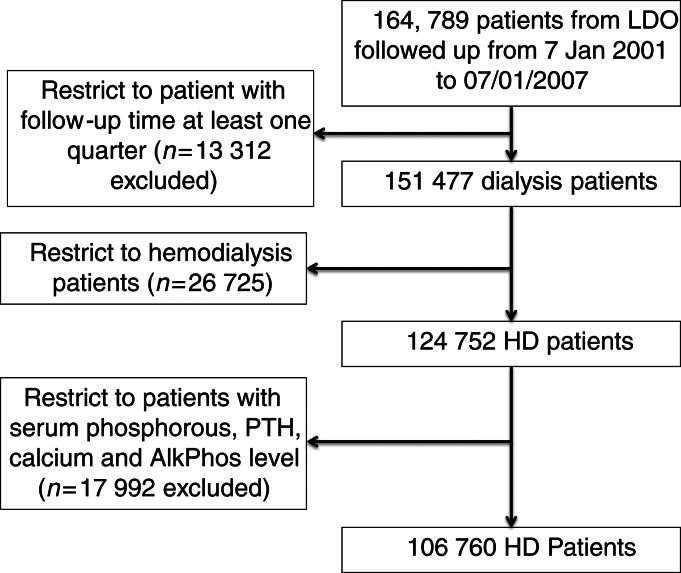
Methods: Over an 8-year period (July 2001-June 2009), we identified 106 760 MHD patients with iPTH and calcium (Ca), phosphorous (P) and ALP data from a large dialysis clinic. Logistic regression models were examined to assess the association between serum iPTH increments and the likelihood of hyperphosphatemia (P ≥5.5 mg/dL), hypercalcemia (Ca ≥10.2 mg/dL) and hyperphosphatasemia (ALP ≥120 U/L).
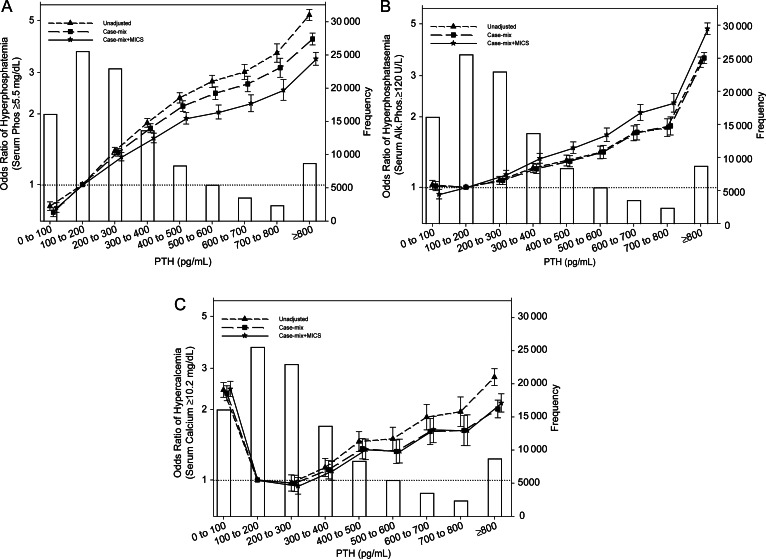
Results: Patients were 61 ± 16 years old and included 45% women, 59% diabetics and 33% Blacks. Compared with an iPTH level of 100 to <200 pg/mL, patients with an iPTH level of 600-700, 700 to <800 and ≥800 pg/mL had 122% (OR: 2.22, 95% CI: 2.04-2.41), 153% (OR: 2.53, 95% CI: 2.29-2.80) and 243% (OR: 3.43, 95% CI: 3.22-3.66) higher risk of hyperphosphatemia, respectively, and had 109% (OR: 2.09, 95% CI: 1.93-2.26), 130% (OR: 2.30, 95% CI: 2.10-2.52) and 376% (OR: 4.76, 95% CI: 4.50-5.04) higher risk of hyperphosphatasemia, respectively. Compared with an iPTH level of 100 to <200 pg/mL, both the low iPTH (<100 pg/mL, OR: 2.45, 95% CI: 2.27-2.64) and the high iPTH (≥800 pg/mL: OR: 2.13, 95% CI: 1.95-2.33) levels were associated with hypercalcemia.
Conclusions: Higher levels of iPTH are incremental correlates of hyperphosphatemia and hyperphosphatasemia, whereas both very low and high PTH levels are linked to hypercalcemia. If these associations are causal, correction of hyperparathyroidism may have overarching implications on bone and mineral disorders in MHD patients.
Keywords: hemodialysis; serum alkaline phosphatase; serum calcium; serum intact parathyroid hormone; serum phosphorous.
Figures
Similar articles
-
The impact of cinacalcet in the mineral metabolism markers of patients on dialysis with severe secondary hyperparathyroidism.J Bras Nefrol. 2019 Jul 18;41(3):336-344. doi: 10.1590/2175-8239-JBN-2018-0219. J Bras Nefrol. 2019. PMID: 31419274 Free PMC article.
-
Treatment of secondary hyperparathyroidism with paricalcitol in patients with end-stage renal disease undergoing hemodialysis in Turkey: an observational study.Int Urol Nephrol. 2019 Jul;51(7):1261-1270. doi: 10.1007/s11255-019-02175-5. Epub 2019 Jun 3. Int Urol Nephrol. 2019. PMID: 31161518
-
19-Nor-1-alpha-25-dihydroxyvitamin D2 (Paricalcitol) safely and effectively reduces the levels of intact parathyroid hormone in patients on hemodialysis.J Am Soc Nephrol. 1998 Aug;9(8):1427-32. doi: 10.1681/ASN.V981427. J Am Soc Nephrol. 1998. PMID: 9697664 Clinical Trial.
-
Renal osteodystrophy in dialysis patients: diagnosis and treatment.Artif Organs. 1998 Jul;22(7):530-57. doi: 10.1046/j.1525-1594.1998.06198.x. Artif Organs. 1998. PMID: 9684690 Review.
-
Alkaline Phosphatase: The Poor Man's iPTH - An Affordable Approach to Bone Health Assessment.J Pak Med Assoc. 2024 Jul;74(7):1374-1375. doi: 10.47391/JPMA.24-52. J Pak Med Assoc. 2024. PMID: 39028076 Review.
Cited by
-
Bone and mineral disorders after kidney transplantation: therapeutic strategies.Transplant Rev (Orlando). 2014 Apr;28(2):56-62. doi: 10.1016/j.trre.2013.12.003. Epub 2013 Dec 12. Transplant Rev (Orlando). 2014. PMID: 24462303 Free PMC article. Review.
-
Recent changes in therapeutic approaches and association with outcomes among patients with secondary hyperparathyroidism on chronic hemodialysis: the DOPPS study.Clin J Am Soc Nephrol. 2015 Jan 7;10(1):98-109. doi: 10.2215/CJN.12941213. Epub 2014 Dec 16. Clin J Am Soc Nephrol. 2015. PMID: 25516917 Free PMC article.
-
Effect Modifying Role of Serum Calcium on Mortality-Predictability of PTH and Alkaline Phosphatase in Hemodialysis Patients: An Investigation Using Data from the Taiwan Renal Registry Data System from 2005 to 2012.PLoS One. 2015 Jun 24;10(6):e0129737. doi: 10.1371/journal.pone.0129737. eCollection 2015. PLoS One. 2015. PMID: 26107510 Free PMC article.
-
Facility-level CKD-MBD composite score and risk of adverse clinical outcomes among patients on hemodialysis.BMC Nephrol. 2016 Nov 4;17(1):166. doi: 10.1186/s12882-016-0382-8. BMC Nephrol. 2016. PMID: 27814753 Free PMC article.
-
Towards the revival of alkaline phosphatase for the management of bone disease, mortality and hip fractures.Nephrol Dial Transplant. 2014 Aug;29(8):1450-2. doi: 10.1093/ndt/gfu086. Epub 2014 Apr 15. Nephrol Dial Transplant. 2014. PMID: 24737443 Free PMC article. Review. No abstract available.
References
-
- Block GA, Klassen PS, Lazarus JM, et al. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004;15:2208–2218. doi:10.1097/01.ASN.0000133041.27682.A2. - DOI - PubMed
-
- Young EW, Albert JM, Satayathum S, et al. Predictors and consequences of altered mineral metabolism: the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2005;67:1179–1187. doi:10.1111/j.1523-1755.2005.00185.x. - DOI - PubMed
-
- Slinin Y, Foley RN, Collins AJ. Calcium, phosphorus, parathyroid hormone, and cardiovascular disease in hemodialysis patients: the USRDS waves 1, 3, and 4 study. J Am Soc Nephrol. 2005;16:1788–1793. doi:10.1681/ASN.2004040275. - DOI - PubMed
-
- Lukowsky LR, Molnar MZ, Zaritsky JJ, et al. Mineral and bone disorders and survival in hemodialysis patients with and without polycystic kidney disease. Nephrol Dial Transplant. 2012;27:2899–2907. doi:10.1093/ndt/gfr747. - DOI - PMC - PubMed
-
- Shantouf R, Kovesdy CP, Kim Y, et al. Association of serum alkaline phosphatase with coronary artery calcification in maintenance hemodialysis patients. Clin J Am Soc Nephrol. 2009;4:1106–1114. doi:10.2215/CJN.06091108. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
