

Lung microbiota and bacterial abundance in patients with bronchiectasis when clinically stable and during exacerbation
- PMID: 23348972
- PMCID: PMC3734618
- DOI: 10.1164/rccm.201210-1937OC
Lung microbiota and bacterial abundance in patients with bronchiectasis when clinically stable and during exacerbation
Abstract
Rationale: Characterization of bacterial populations in infectious respiratory diseases will provide improved understanding of the relationship between the lung microbiota, disease pathogenesis, and treatment outcomes.
Objectives: To comprehensively define lung microbiota composition during stable disease and exacerbation in patients with bronchiectasis.
Methods: Sputum was collected from patients when clinically stable and before and after completion of antibiotic treatment of exacerbations. Bacterial abundance and community composition were analyzed using anaerobic culture and 16S rDNA pyrosequencing.
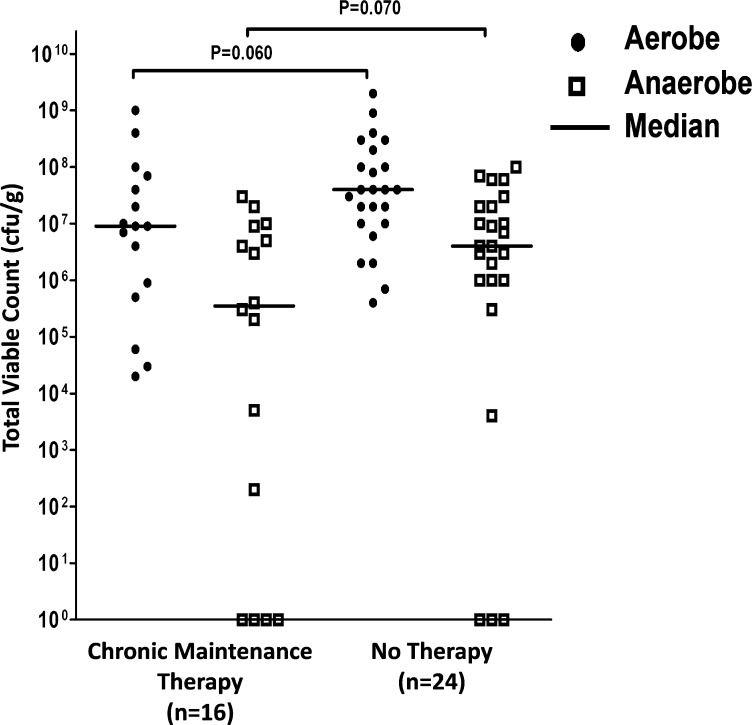
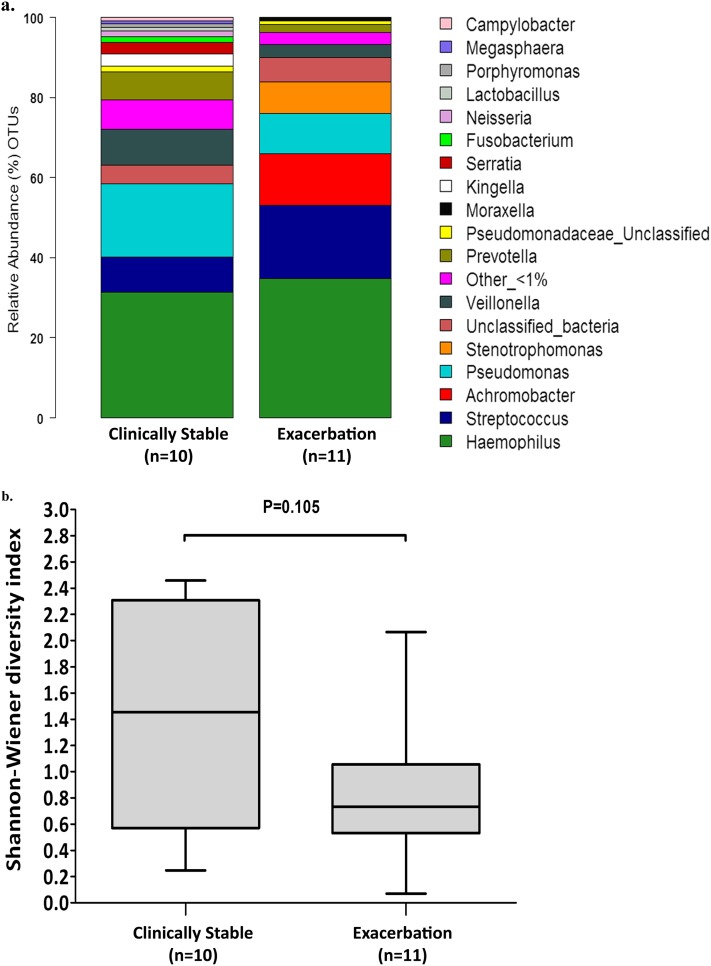
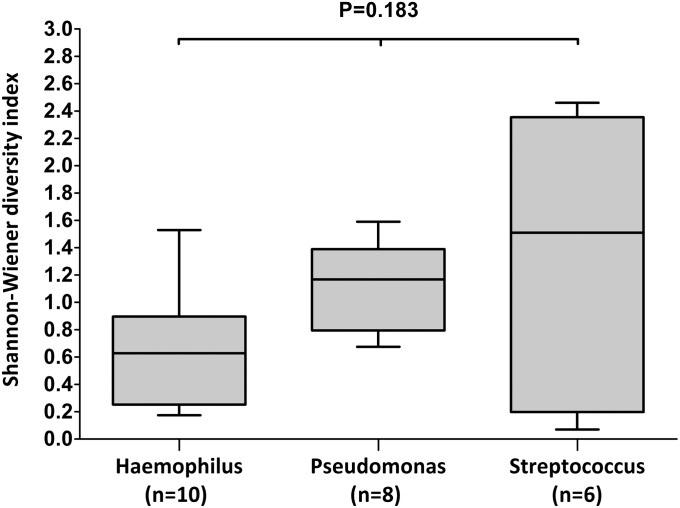
Measurements and main results: In clinically stable patients, aerobic and anaerobic bacteria were detected in 40 of 40 (100%) and 33 of 40 (83%) sputum samples, respectively. The dominant organisms cultured were Pseudomonas aeruginosa (n = 10 patients), Haemophilus influenzae (n = 12), Prevotella (n = 18), and Veillonella (n = 13). Pyrosequencing generated more than 150,000 sequences, representing 113 distinct microbial taxa; the majority of observed community richness resulted from taxa present in low abundance with similar patterns of phyla distribution in clinically stable patients and patients at the onset of exacerbation. After treatment of exacerbation, there was no change in total (P = 0.925), aerobic (P = 0.917), or anaerobic (P = 0.683) load and only a limited shift in community composition. Agreement for detection of bacteria by culture and pyrosequencing was good for aerobic bacteria such as P. aeruginosa (κ = 0.84) but poorer for other genera including anaerobes. Lack of agreement was largely due to bacteria being detected by pyrosequencing but not by culture.
Conclusions: A complex microbiota is present in the lungs of patients with bronchiectasis and remains stable through treatment of exacerbations, suggesting that changes in microbiota composition do not account for exacerbations.
Figures



Comment in
-
Microbes in bronchiectasis: the forest or the trees?Am J Respir Crit Care Med. 2013 May 15;187(10):1044-5. doi: 10.1164/rccm.201302-0240ED. Am J Respir Crit Care Med. 2013. PMID: 23675713 No abstract available.
References
-
- Barker AF. Bronchiectasis. N Engl J Med. 2002;346:1383–1393. - PubMed
-
- Martínez-García MA, Soler-Cataluña J-J, Perpiñá-Tordera M, Román-Sánchez P, Soriano J. Factors associated with lung function decline in adult patients with stable non–cystic fibrosis bronchiectasis. Chest. 2007;132:1565–1572. - PubMed
-
- Evans DJ, Greenstone M. Long-term antibiotics in the management of non-CF bronchiectasis—do they improve outcome? Respir Med. 2003;97:851–858. - PubMed
-
- Martínez-García MA, Perpiñá-Tordera M, Román-Sánchez P, Soler-Cataluña JJ. Quality-of-life determinants in patients with clinically stable bronchiectasis. Chest. 2005;128:739–745. - PubMed
-
- Wilson CB, Jones PW, O’Leary CJ, Hansell DM, Cole PJ, Wilson R. Effect of sputum bacteriology on the quality of life of patients with bronchiectasis. Eur Respir J. 1997;10:1754–1760. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
