

Fungal interface keratitis by Candida orthopsilosis following deep anterior lamellar keratoplasty
- PMID: 23349184
- PMCID: PMC3604172
- DOI: 10.1136/bcr-2012-008361
Fungal interface keratitis by Candida orthopsilosis following deep anterior lamellar keratoplasty
Abstract
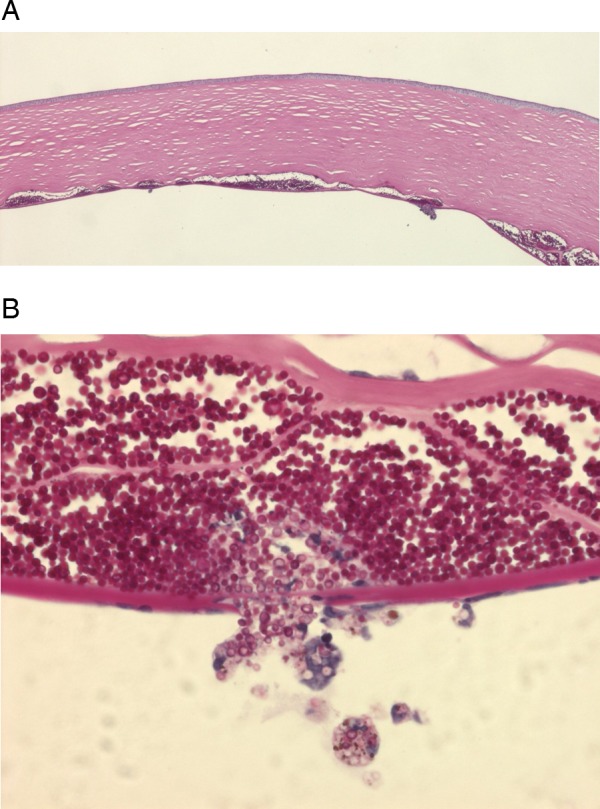
A 39-year-old male patient underwent uncomplicated deep anterior lamellar keratoplasty due to keratoconus. On day 5 after surgery, small whitish infiltrates developed in the corneal interface. The diagnosis of fungal keratitis was made when the culture medium of the graft grew Candida after the surgical intervention. Despite intensive antimycotic treatment and irrigation of the interface, the infiltrates persisted and eventually enlarged. Therefore, revision surgery with penetrating keratoplasty was performed. Microbiological analysis showed Candida orthopsilosis in the culture of the excised graft button. Histopathological staining of the excised graft showed periodic acid-Schiff-positive and Grocott methenamine silver-positive clusters of yeast between Descemet's membrane and the deep corneal stroma with focal perforations through Descemet's membrane. The treatment of mycotic keratitis caused by C orthopsilosis is challenging. Antimycotic treatment was unsuccessful in this case. Progression of the keratitis and perforation of Descemet's membrane suggest that early surgical intervention by penetrating keratoplasty is required.
Figures



References
-
- Anwar M, Teichmann KD. Big-bubble technique to bare Descemet's membrane in anterior lamellar keratoplasty. J Cataract Refract Surg 2002;28:398–403 - PubMed
-
- Kanavi MR, Foroutan AR, Kamel MR, et al. Candida interface keratitis after deep anterior lamellar keratoplasty: clinical, microbiologic, histopathologic, and confocal microscopic reports. Cornea 2007;26:913–16 - PubMed
-
- Fontana L, Parente G, Di Pede B, et al. Candida albicans interface infection after deep anterior lamellar keratoplasty. Cornea 2007;26:883–5 - PubMed
-
- Bahadir AE, Bozkurt TK, Kutan SA, et al. Candida interface keratitis following deep anterior lamellar keratoplasty. Int Ophthalmol 2012;32:383–6 - PubMed
-
- Fintelmann RE, Gilmer W, Bloomer MM, et al. Recurrent Lecythophora mutabilis keratitis and endophthalmitis after deep anterior lamellar keratoplasty. Arch Ophthalmol 2011;129:108–10 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources