

Maternal and fetal risk factors for stillbirth: population based study
- PMID: 23349424
- PMCID: PMC3554866
- DOI: 10.1136/bmj.f108
Maternal and fetal risk factors for stillbirth: population based study
Abstract
Objective: To assess the main risk factors associated with stillbirth in a multiethnic English maternity population.
Design: Cohort study.
Setting: National Health Service region in England.
Population: 92,218 normally formed singletons including 389 stillbirths from 24 weeks of gestation, delivered during 2009-11.
Main outcome measure: Risk of stillbirth.
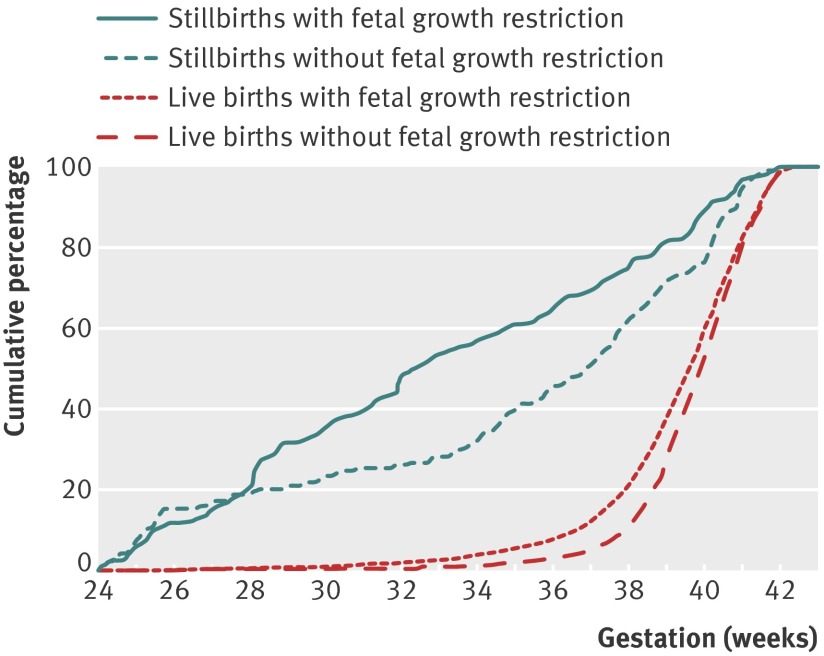
Results: Multivariable analysis identified a significant risk of stillbirth for parity (para 0 and para ≥ 3), ethnicity (African, African-Caribbean, Indian, and Pakistani), maternal obesity (body mass index ≥ 30), smoking, pre-existing diabetes, and history of mental health problems, antepartum haemorrhage, and fetal growth restriction (birth weight below 10th customised birthweight centile). As potentially modifiable risk factors, maternal obesity, smoking in pregnancy, and fetal growth restriction together accounted for 56.1% of the stillbirths. Presence of fetal growth restriction constituted the highest risk, and this applied to pregnancies where mothers did not smoke (adjusted relative risk 7.8, 95% confidence interval 6.6 to 10.9), did smoke (5.7, 3.6 to 10.9), and were exposed to passive smoke only (10.0, 6.6 to 15.8). Fetal growth restriction also had the largest population attributable risk for stillbirth and was fivefold greater if it was not detected antenatally than when it was (32.0% v 6.2%). In total, 195 of the 389 stillbirths in this cohort had fetal growth restriction, but in 160 (82%) it had not been detected antenatally. Antenatal recognition of fetal growth restriction resulted in delivery 10 days earlier than when it was not detected: median 270 (interquartile range 261-279) days v 280 (interquartile range 273-287) days. The overall stillbirth rate (per 1000 births) was 4.2, but only 2.4 in pregnancies without fetal growth restriction, increasing to 9.7 with antenatally detected fetal growth restriction and 19.8 when it was not detected.
Conclusion: Most normally formed singleton stillbirths are potentially avoidable. The single largest risk factor is unrecognised fetal growth restriction, and preventive strategies need to focus on improving antenatal detection.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Identifying risk factors for stillbirth.BMJ. 2013 Jan 24;346:f416. doi: 10.1136/bmj.f416. BMJ. 2013. PMID: 23349425 No abstract available.
-
Increase in stillbirths in Greece is linked to the economic crisis.BMJ. 2013 Feb 19;346:f1061. doi: 10.1136/bmj.f1061. BMJ. 2013. PMID: 23423369 No abstract available.
References
-
- Saving Babies Lives Report. Stillbirth and Neonatal Death Charity (SANDS), 2009. 2012. www.why17.org/fileadmin/content/About_Sands/03520_Saving_babies_lives_wa....
-
- Flenady V, Middleton P, Smith GC, Duke W, Erwich JJ, Yee Khong T, et al. Stillbirths: the way forward in high-income countries. Lancet 2011;377:1703-17. - PubMed
-
- Office for National Statistics (2011). Death registration summary tables, England & Wales, 2010. 2012. www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A7....
-
- Confidential Enquiry into Maternal and Child Health (CEMACH). Perinatal mortality 2006: England, Wales and Northern Ireland. CEMACH, 2008. (Table 4.2).
-
- Gardosi J. Clinical implications of ‘unexplained’ stillbirths. In: Maternal and Child Health Research Consortium, ed: CESDI 8th annual report.Confidential Enquiry into Stillbirths and Deaths in Infancy, 2001:40-7.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials