

The effect of real-time continuous glucose monitoring in pregnant women with diabetes: a randomized controlled trial
- PMID: 23349548
- PMCID: PMC3687305
- DOI: 10.2337/dc12-2360
The effect of real-time continuous glucose monitoring in pregnant women with diabetes: a randomized controlled trial
Abstract
Objective: To assess whether intermittent real-time continuous glucose monitoring (CGM) improves glycemic control and pregnancy outcome in unselected women with pregestational diabetes.
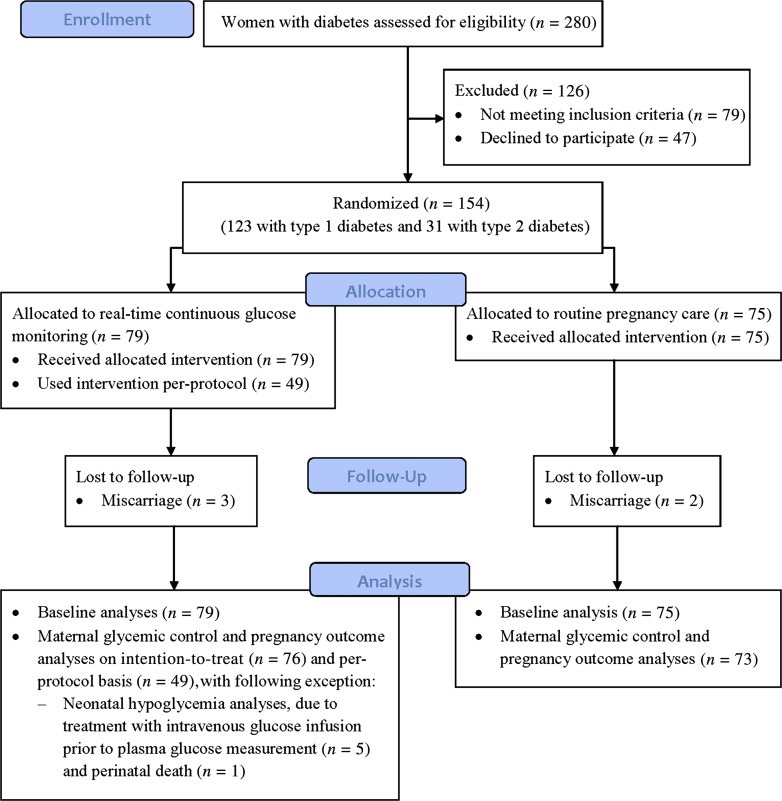
Research design and methods: A total of 123 women with type 1 diabetes and 31 women with type 2 diabetes were randomized to use real-time CGM for 6 days at 8, 12, 21, 27, and 33 weeks in addition to routine care, including self-monitored plasma glucose seven times daily, or routine care only. To optimize glycemic control, real-time CGM readings were evaluated by a diabetes caregiver. HbA1c, self-monitored plasma glucose, severe hypoglycemia, and pregnancy outcomes were recorded, with large-for-gestational-age infants as the primary outcome.
Results: Women assigned to real-time CGM (n = 79) had baseline HbA1c similar to that of women in the control arm (n = 75) (median 6.6 [range 5.3-10.0] vs. 6.8% [5.3-10.7]; P = 0.67) (49 [34-86] vs. 51 mmol/mol [34-93]). Forty-nine (64%) women used real-time CGM per protocol. At 33 weeks, HbA1c (6.1 [5.1-7.8] vs. 6.1% [4.8-8.2]; P = 0.39) (43 [32-62] vs. 43 mmol/mol [29-66]) and self-monitored plasma glucose (6.2 [4.7-7.9] vs. 6.2 mmol/L [4.9-7.9]; P = 0.64) were comparable regardless of real-time CGM use, and a similar fraction of women had experienced severe hypoglycemia (16 vs. 16%; P = 0.91). The prevalence of large-for-gestational-age infants (45 vs. 34%; P = 0.19) and other perinatal outcomes were comparable between the arms.
Conclusions: In this randomized trial, intermittent use of real-time CGM in pregnancy, in addition to self-monitored plasma glucose seven times daily, did not improve glycemic control or pregnancy outcome in women with pregestational diabetes.
Trial registration: ClinicalTrials.gov NCT00994357.
Figures
Comment in
-
Continuous glucose monitoring in pregnancy: we have the technology but not all the answers.Diabetes Care. 2013 Jul;36(7):1818-9. doi: 10.2337/dc13-0273. Diabetes Care. 2013. PMID: 23801793 Free PMC article. No abstract available.
References
-
- de Valk HW, Visser GH. Insulin during pregnancy, labour and delivery. Best Pract Res Clin Obstet Gynaecol 2011;25:65–76 - PubMed
-
- Klemetti M, Nuutila M, Tikkanen M, Kari MA, Hiilesmaa V, Teramo K. Trends in maternal BMI, glycaemic control and perinatal outcome among type 1 diabetic pregnant women in 1989-2008. Diabetologia 2012;55:2327–2334 - PubMed
-
- Mathiesen ER, Vaz JA. Insulin treatment in diabetic pregnancy. Diabetes Metab Res Rev 2008;24(Suppl. 2):S3–S20 - PubMed
-
- Persson M, Pasupathy D, Hanson U, Norman M. Disproportionate body composition and perinatal outcome in large-for-gestational-age infants to mothers with type 1 diabetes. BJOG 2012;119:565–572 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
