

Epidemiology, microbiology and mortality associated with community-acquired bacteremia in northeast Thailand: a multicenter surveillance study
- PMID: 23349954
- PMCID: PMC3548794
- DOI: 10.1371/journal.pone.0054714
Epidemiology, microbiology and mortality associated with community-acquired bacteremia in northeast Thailand: a multicenter surveillance study
Erratum in
- PLoS One. 2013;8(10). doi:10.1371/annotation/e199ebcc-0bc1-4be1-ad91-ad2a8c0c9382
Abstract
Background: National statistics in developing countries are likely to underestimate deaths due to bacterial infections. Here, we calculated mortality associated with community-acquired bacteremia (CAB) in a developing country using routinely available databases.
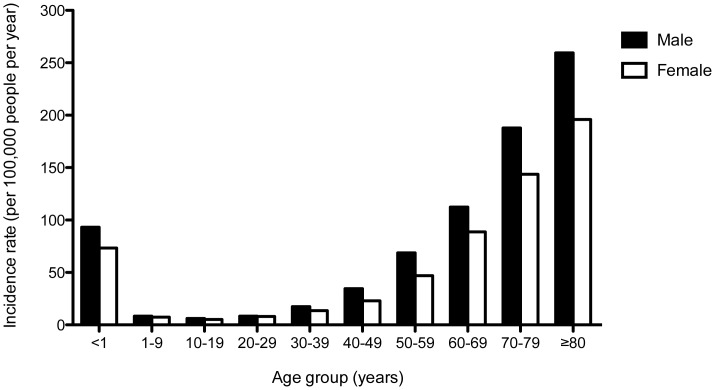
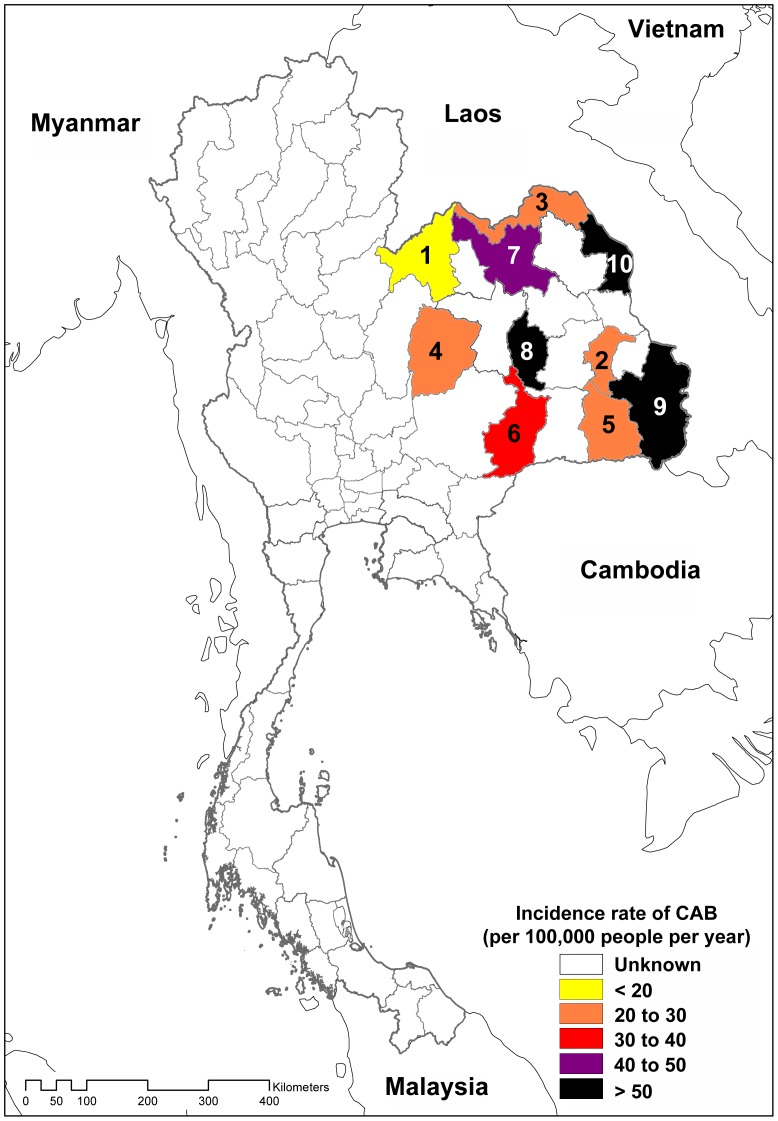
Methods/principal findings: Information was obtained from the microbiology and hospital database of 10 provincial hospitals in northeast Thailand, and compared with the national death registry from the Ministry of Interior, Thailand for the period between 2004 and 2010. CAB was defined in patients who had pathogenic organisms isolated from blood taken within 2 days of hospital admission without a prior inpatient episode in the preceding 30 days. A total of 15,251 CAB patients identified, of which 5,722 (37.5%) died within 30 days of admission. The incidence rate of CAB between 2004 and 2010 increased from 16.7 to 38.1 per 100,000 people per year, and the mortality rate associated with CAB increased from 6.9 to 13.7 per 100,000 people per year. In 2010, the mortality rate associated with CAB was lower than that from respiratory tract infection, but higher than HIV disease or tuberculosis. The most common causes of CAB were Escherichia coli (23.1%), Burkholderia pseudomallei (19.3%), and Staphylococcus aureus (8.2%). There was an increase in the proportion of Extended-Spectrum Beta-Lactamases (ESBL) producing E. coli and Klebsiella pneumoniae over time.
Conclusions: This study has demonstrated that national statistics on causes of death in developing countries could be improved by integrating information from readily available databases. CAB is neglected as an important cause of death, and specific prevention and intervention is urgently required to reduce its incidence and mortality.
Conflict of interest statement
Figures

References
-
- Pedersen G, Schonheyder HC, Sorensen HT (2003) Source of infection and other factors associated with case fatality in community-acquired bacteremia–a Danish population-based cohort study from 1992 to 1997. Clinical microbiology and infection 9: 793–802. - PubMed
-
- Sogaard M, Norgaard M, Dethlefsen C, Schonheyder HC (2011) Temporal changes in the incidence and 30-day mortality associated with bacteremia in hospitalized patients from 1992 through 2006: a population-based cohort study. Clinical infectious diseases 52: 61–69. - PubMed
-
- Uslan DZ, Crane SJ, Steckelberg JM, Cockerill FR 3rd, St Sauver JL, et al. (2007) Age- and sex-associated trends in bloodstream infection: a population-based study in Olmsted County, Minnesota. Archives of internal medicine 167: 834–839. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
