Computed tomography mimics of acute appendicitis: predictors of appendiceal disease confirmed at pathology
- PMID: 23350063
- PMCID: PMC3551488
- DOI: 10.4103/2156-7514.104306
Computed tomography mimics of acute appendicitis: predictors of appendiceal disease confirmed at pathology
Abstract
Purpose: Imaging and pathology findings are used to analyze the capability of computed tomography (CT) to distinguish between acute appendicitis and radiological mimickers.
Materials and methods: A retrospective review of 5861 patients undergoing abdominopelvic CT from 2000 to 2008 for suspicion of acute appendicitis was performed. Appendix diameter, surrounding inflammation, appendicolith, and location were assessed. Only those cases were included where patients underwent surgery for acute appendicitis on CT findings. Pathology specimens were examined and those indicative of acute appendicitis were identified. Statistical analysis was performed to correlate pathology and CT signs.
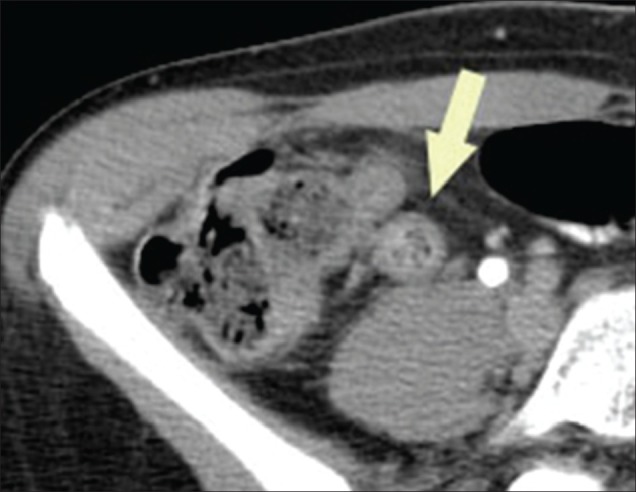
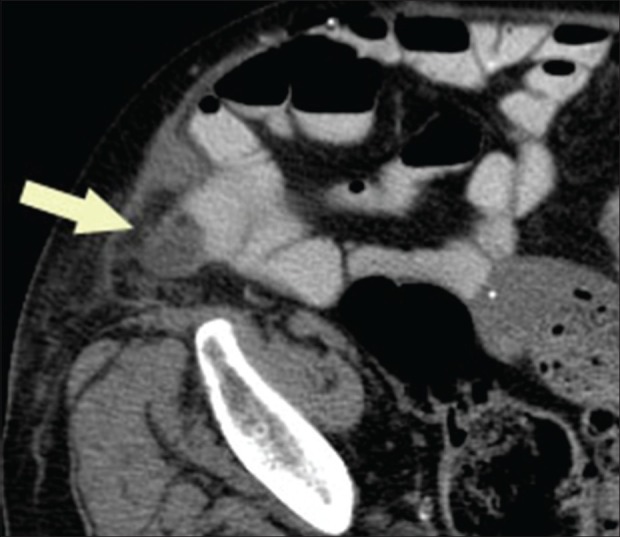
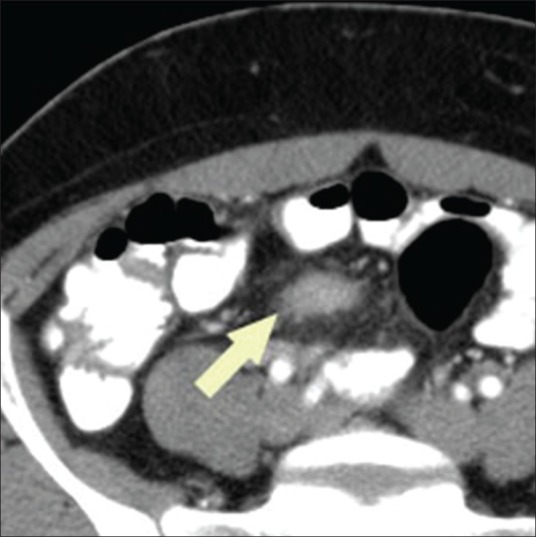
Results: A total of 969 of the 5681 patients were included in the study. Acute appendicitis was verified in 870/969 (89%) cases, while 99/969 (11%) demonstrated either chronic findings (i.e., fibrosis [32%], granulomatous disease [16%], lymphoid hyperplasia [11%]) or no abnormality. In regression models, appendiceal diameter >7 mm (odds ratio [OR] = 3.98, P < 0.0001) and mesenteric fat stranding (OR = 6.04, P < 0.0001) were associated with acute appendicitis. Nearly 87% (754/870) of acute appendicitis cases showed both signs on CT, compared with 53% (52/99) of those with other pathologic finding (P < 0.0001). In cases with non-appendicitis findings, 39% (39/99) had only one of these signs compared with 13% (112/870) of those with acute appendicitis (P < 0.0001).
Conclusion: Diseases of the appendix other than acute appendicitis may manifest with isolated radiological findings and should be considered as part of the differential diagnosis in cases of borderline acute appendicitis.
Keywords: Abdominal radiology; appendicitis; computed tomography.
Conflict of interest statement
Figures
References
-
- Lane MJ, Liu DM, Huynh MD, Jeffrey RB, Jr, Mindelzun RE, Katz DS. Suspected acute appendicitis: nonenhanced helical CT in 300 consecutive patients. Radiology. 1999;213:341–6. - PubMed
-
- Choi YH, Fischer E, Hoda SA, Rubenstein WA, Morrissey KP, Hertford D, et al. Appendiceal CT in 140 cases: Diagnostic criteria for acute and necrotizing appendicitis. Clin Imaging. 1998;22:252–71. - PubMed
-
- Raja AS, Wright C, Sodickson AD, Zane RD, Schiff GD, Hanson R, et al. Negative appendectomy in the era of CT: An 18 year perspective. Radiology. 2010;256:460–5. - PubMed
-
- Bendeck SE, Nino-Murcia M, Berry GJ, Jeffery RB. Imaging for suspected appendicitis: Negative appendectomy and perforation rates. Radiology. 2002;225:131–6. - PubMed
LinkOut - more resources
Full Text Sources