

Identifying the translational gap in the evaluation of drug-induced QTc interval prolongation
- PMID: 23351036
- PMCID: PMC3853530
- DOI: 10.1111/bcp.12082
Identifying the translational gap in the evaluation of drug-induced QTc interval prolongation
Abstract
Aims: Given the similarities in QTc response between dogs and humans, dogs are used in pre-clinical cardiovascular safety studies. The objective of our investigation was to characterize the PKPD relationships and identify translational gaps across species following the administration of three compounds known to cause QTc interval prolongation, namely cisapride, d, l-sotalol and moxifloxacin.
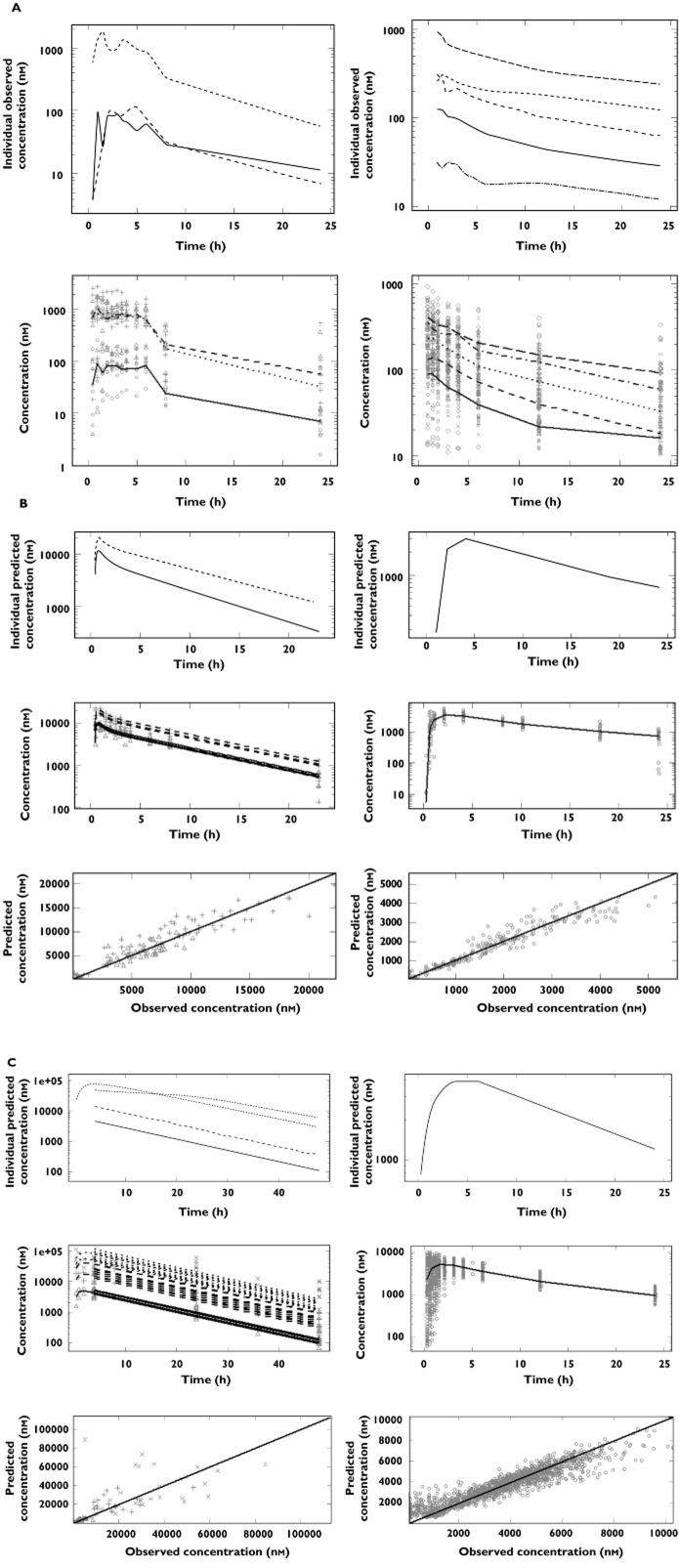
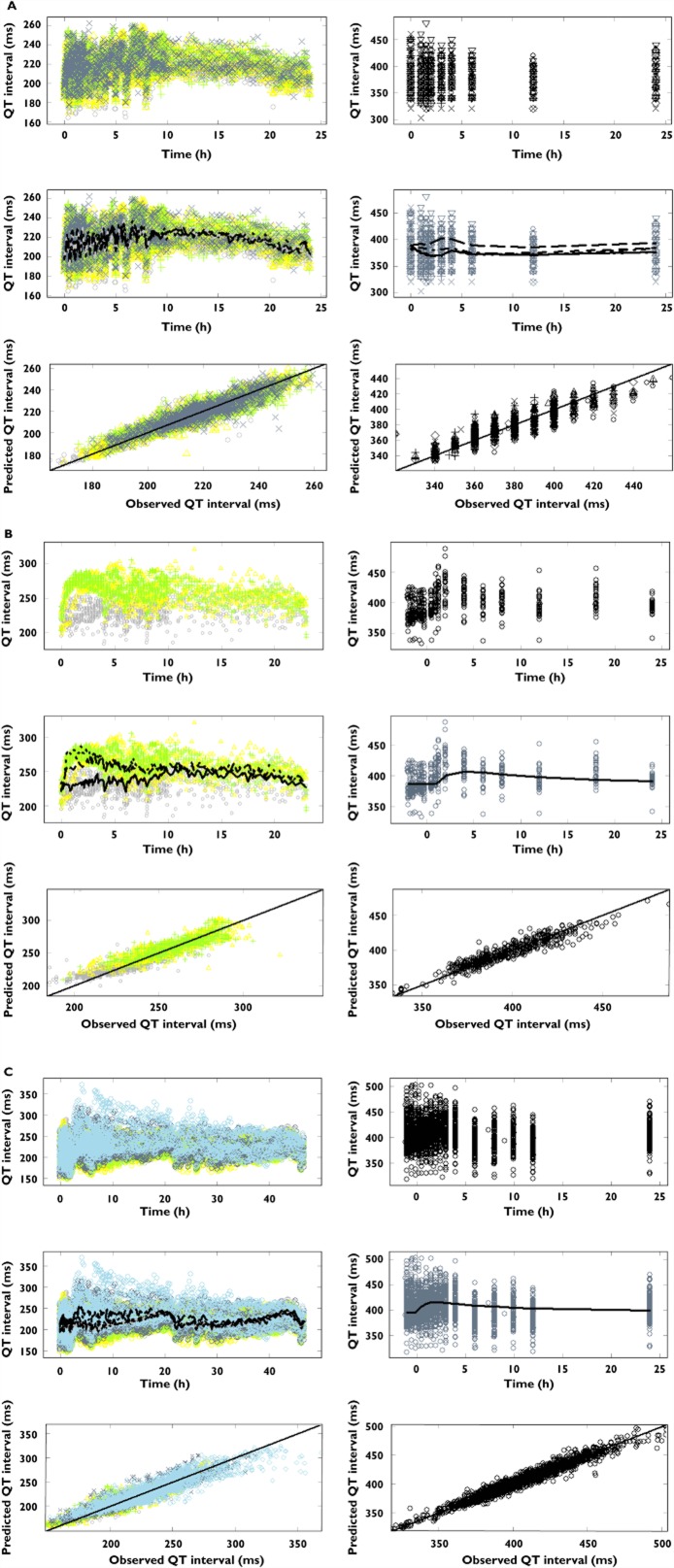
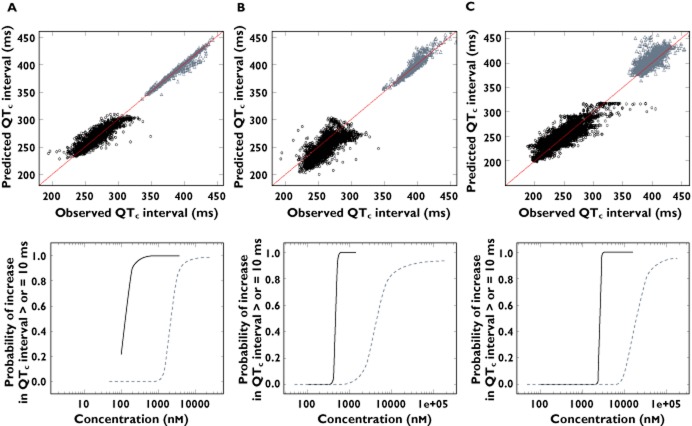
Methods: Pharmacokinetic and pharmacodynamic data from experiments in conscious dogs and clinical trials were included in this analysis. First, pharmacokinetic modelling and deconvolution methods were applied to derive drug concentrations at the time of each QT measurement. A Bayesian PKPD model was then used to describe QT prolongation, allowing discrimination of drug-specific effects from other physiological factors known to alter QT interval duration. A threshold of ≥10 ms was used to explore the probability of prolongation after drug administration.
Results: A linear relationship was found to best describe the pro-arrhythmic effects of cisapride, d,l-sotalol and moxifloxacin both in dogs and in humans. The drug-specific parameter (slope) in dogs was statistically significantly different from humans. Despite such differences, our results show that the probability of QTc prolongation ≥10 ms in dogs nears 100% for all three compounds at the therapeutic exposure range in humans.
Conclusions: Our findings indicate that the slope of PKPD relationship in conscious dogs may be used as the basis for the prediction of drug-induced QTc prolongation in humans. Furthermore, the risk of QTc prolongation can be expressed in terms of the probability associated with an increase ≥10 ms, allowing direct inferences about the clinical relevance of the pro-arrhythmic potential of a molecule.
Keywords: QTc interval prolongation; model-based drug development; pre-clinical studies; translational science.
© 2013 The Authors. British Journal of Clinical Pharmacology © 2013 The British Pharmacological Society.
Figures
References
-
- Darpo B, Nebout T, Sager PT. Clinical evaluation of QT/QTc prolongation and proarrhythmic potential for nonantiarrhythmic drugs: the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use E14 guideline. J Clin Pharmacol. 2006;46:498–507. - PubMed
-
- ICH Expert Working Group. ICH Harmonised tripartite guideline. E14 Clinical Evaluation of QT/QTc Interval Prolongation and Proarrythmic Potential for Non-Antiarrythmic. Drugs. 2005
-
- Danhof M, de Lange EC, Della Pasqua OE, Ploeger BA, Voskuyl RA. Mechanism-based pharmacokinetic-pharmacodynamic (PK-PD) modeling in translational drug research. Trends Pharmacol Sci. 2008;29:186–191. - PubMed
-
- ICH Expert Working Group. ICH Harmonised tripartite guideline. S7A Safety pharmacology studies for human pharmaceuticals, 2000.
-
- ICH Expert Working Group. ICH Harmonised tripartite guideline. S7B The nonclinical evaluation of the potential for delayed ventricular repolarization (QT interval prolongation) by human pharmaceuticals, 2005. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
