

Comparative efficacy and tolerability of anti-epileptic drugs for refractory focal epilepsy: systematic review and network meta-analysis reveals the need for long term comparator trials
- PMID: 23351090
- PMCID: PMC3853525
- DOI: 10.1111/bcp.12083
Comparative efficacy and tolerability of anti-epileptic drugs for refractory focal epilepsy: systematic review and network meta-analysis reveals the need for long term comparator trials
Abstract
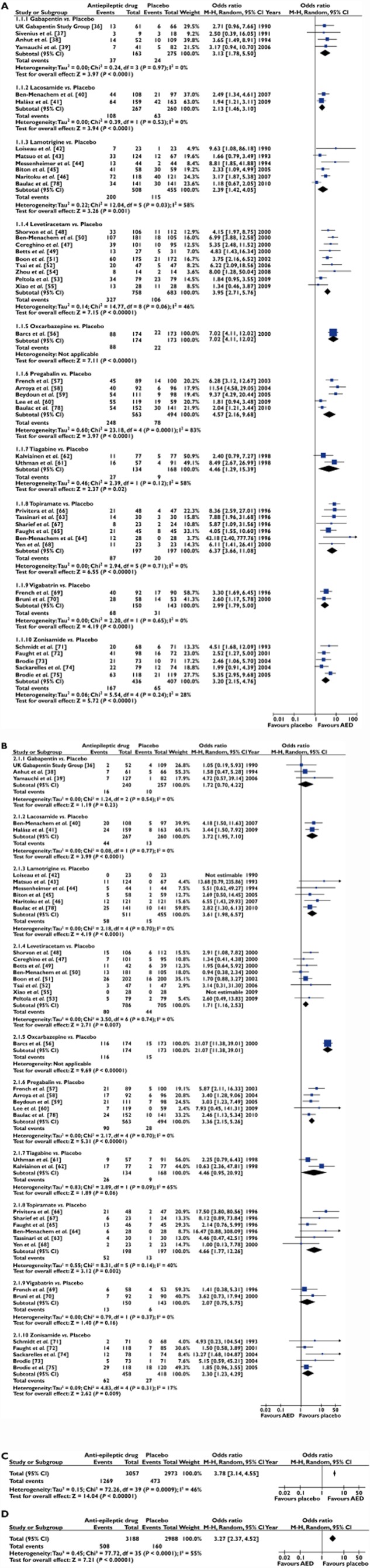
Aims: To evaluate the comparative efficacy (50% reduction in seizure frequency) and tolerability (premature withdrawal due to adverse events) of anti-epileptic drugs (AEDs) for refractory epilepsy.
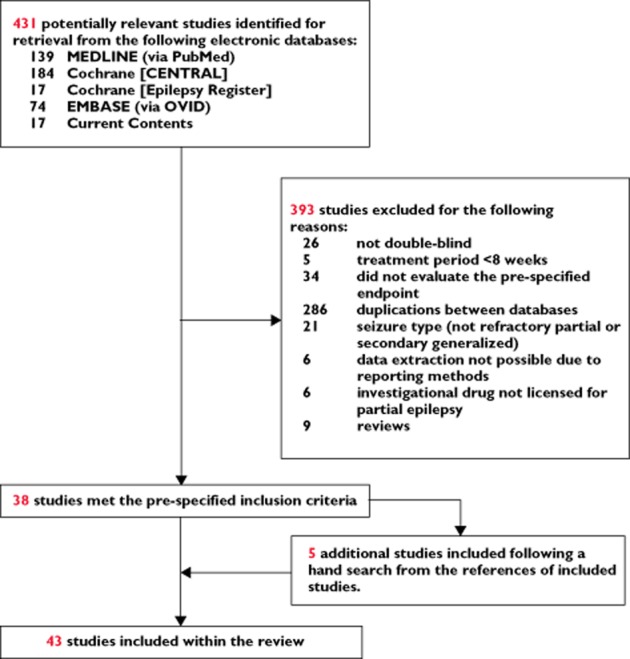
Methods: We searched Cochrane Central Register of Controlled Trials (Cochrane Library 2009, issue 2) including Epilepsy Group's specialized register, MEDLINE (1950 to March 2009), EMBASE (1980 to March 2009), and Current Contents Connect (1998 to March 2009) to conduct a systematic review of published studies, developed a treatment network and undertook a network meta-analysis.
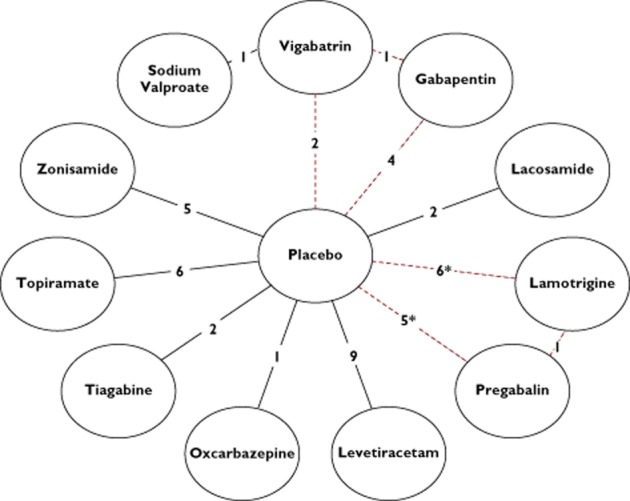
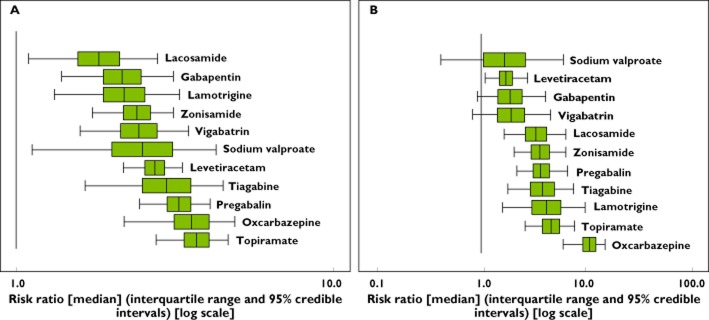
Results: Forty-three eligible trials with 6346 patients and 12 interventions, including placebo, contributed to the analysis. Only three direct drug comparator trials were identified, the remaining 40 trials being placebo-controlled. Conventional random-effects meta-analysis indicated all drugs were superior in efficacy to placebo (overall odds ratio (OR] 3.78, 95% CI 3.14, 4.55) but did not permit firm distinction between drugs on the basis of the efficacy or tolerability. A Bayesian network meta-analysis prioritized oxcarbazepine, topiramate and pregabalin on the basis of short term efficacy. However, sodium valproate, levetiracetam, gabapentin and vigabatrin were prioritized on the basis of short-term efficacy and tolerability, with the caveat that vigabatrin is recognized as being associated with serious visual disturbance with chronic use.
Conclusion: Of the wide range of AEDs licensed for the treatment of refractory epilepsy, sodium valproate, levetiracetam and gabapentin demonstrated the best balance of efficacy and tolerability. Until regulators mandate greater use of active comparator trials with longer term follow-up, network meta-analysis provides the only available means to quantify these clinically important parameters.
Keywords: anticonvulsants/therapeutic use; comparative study; epilepsy/drug therapy; meta-analysis; review; treatment outcome.
© 2013 The Authors. British Journal of Clinical Pharmacology © 2013 The British Pharmacological Society.
Figures
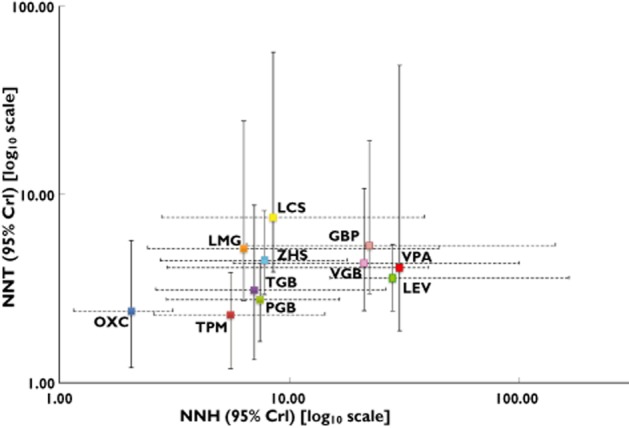
 , gabapentin (GBP);
, gabapentin (GBP);  , lacosamide (LCS);
, lacosamide (LCS);  , lamotrigine (LMG);
, lamotrigine (LMG);  , levetiracetam (LEV);
, levetiracetam (LEV);  , oxcarbazepine (OXC);
, oxcarbazepine (OXC);  , pregabalin (PGB);
, pregabalin (PGB);  , sodium valproate (VPA);
, sodium valproate (VPA);  , tiagabine (TGB);
, tiagabine (TGB);  , topiramate (TPM);
, topiramate (TPM);  , vigabatrin (VGB);
, vigabatrin (VGB);  , zonisamide (ZNS)
, zonisamide (ZNS)Comment in
-
Network meta-analysis and the comparison of efficacy and tolerability of anti-epileptic drugs for treatment of refractory focal epilepsy.Br J Clin Pharmacol. 2013 Nov;76(5):827-8. doi: 10.1111/bcp.12175. Br J Clin Pharmacol. 2013. PMID: 23738499 Free PMC article. No abstract available.
References
-
- Blume WT. Glossary of descriptive terminology for ictal semiology: report of the ILAE Task Force on Classification and Terminology. Epilepsia. 2001;42:1212–1218. - PubMed
-
- World Health Organization. 2009. Epilepsy. Fact Sheet number 999.
-
- Shorvon SD. The epidemiology and treatment of chronic and refractory epilepsy. Epilepsia. 1996;37:S1–S3. - PubMed
-
- Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Hauser WA, Mathern G, Moshe SL, Perucca E, Wiebe S, French J. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51:1069–1077. - PubMed
-
- Cockerell OC, Sander JWAS, Hart YM, Shorvon SD, Johnson AL. Remission of epilepsy: results from the National General Practice Study of Epilepsy. Lancet. 1995;346:140–144. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
