

Severe lower respiratory tract infection in infants and toddlers from a non-affluent population: viral etiology and co-detection as risk factors
- PMID: 23351117
- PMCID: PMC3598993
- DOI: 10.1186/1471-2334-13-41
Severe lower respiratory tract infection in infants and toddlers from a non-affluent population: viral etiology and co-detection as risk factors
Abstract
Background: Lower respiratory tract infection (LRTI) is a major cause of pediatric morbidity and mortality, especially among non-affluent communities. In this study we determine the impact of respiratory viruses and how viral co-detections/infections can affect clinical LRTI severity in children in a hospital setting.
Methods: Patients younger than 3 years of age admitted to a tertiary hospital in Brazil during the months of high prevalence of respiratory viruses had samples collected from nasopharyngeal aspiration. These samples were tested for 13 different respiratory viruses through real-time PCR (rt-PCR). Patients were followed during hospitalization, and clinical data and population characteristics were collected during that period and at discharge to evaluate severity markers, especially length of hospital stay and oxygen use. Univariate regression analyses identified potential risk factors and multivariate logistic regressions were used to determine the impact of specific viral detections as well as viral co-detections in relation to clinical outcomes.
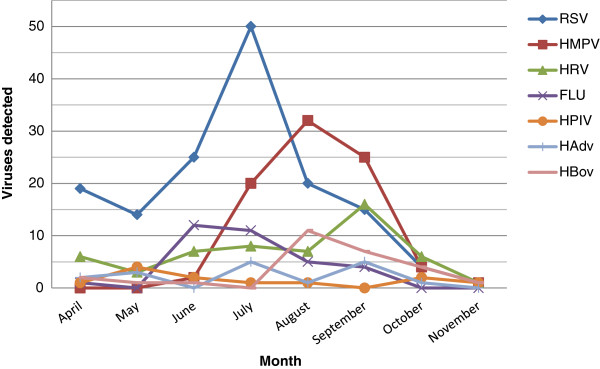
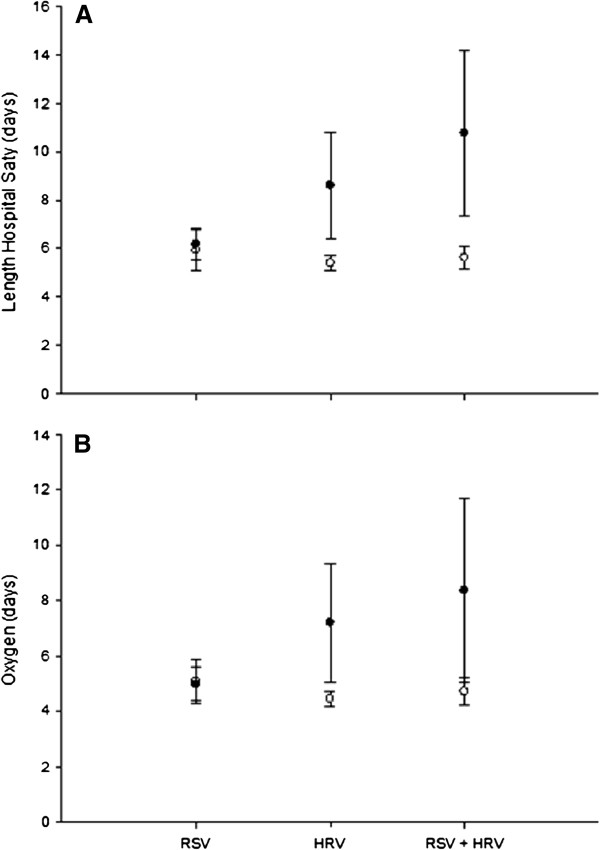
Results: We analyzed 260 episodes of LRTI with a viral detection rate of 85% (n = 222). Co-detection was observed in 65% of all virus-positive episodes. The most prevalent virus was Respiratory Syncytial Virus (RSV) (54%), followed by Human Metapneumovirus (hMPV) (32%) and Human Rhinovirus (HRV) (21%). In the multivariate models, infants with co-detection of HRV + RSV stayed 4.5 extra days (p = 0.004), when compared to infants without the co-detection. The same trends were observed for the outcome of days of supplemental oxygen use.
Conclusions: Although RSV remains as the main cause of LRTI in infants our study indicates an increase in the length of hospital stay and oxygen use in infants with HRV detected by RT-PCR compared to those without HRV. Moreover, one can speculate that when HRV is detected simultaneously with RSV there is an additive effect that may be reflected in more severe clinical outcome. Also, our study identified a significant number of children infected by recently identified viruses, such as hMPV and Human Bocavirus (HBov), and this is a novel finding for poor communities from developing countries.
Figures
References
-
- Global action plan for prevention and control of pneumonia (GAPP) http://www.who.int/maternal_child_adolescent/documents/9789241596336/en/ - PMC - PubMed
-
- Freymuth F, Vabret A, Cuvillon-Nimal D, Simon S, Dina J, Legrand L, Gouarin S, Petitjean J, Eckart P, Brouard J. Comparison of multiplex PCR assays and conventional techniques for the diagnostic of respiratory virus infections in children admitted to hospital with an acute respiratory illness. J Med Virol. 2006;78(11):1498–1504. doi: 10.1002/jmv.20725. - DOI - PMC - PubMed
-
- Nair H, Nokes DJ, Gessner BD, Dherani M, Madhi SA, Singleton RJ, O’Brien KL, Roca A, Wright PF, Bruce N. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet. 2010;375(9725):1545–1555. doi: 10.1016/S0140-6736(10)60206-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
