

Reducing elective general surgery cancellations at a Canadian hospital
- PMID: 23351498
- PMCID: PMC3617116
- DOI: 10.1503/cjs.018411
Reducing elective general surgery cancellations at a Canadian hospital
Abstract
Background: In Canadian hospitals, which are typically financed by global annual budgets, overuse of operating rooms is a financial risk that is frequently managed by cancelling elective surgical procedures. It is uncertain how different scheduling rules affect the rate of elective surgery cancellations.
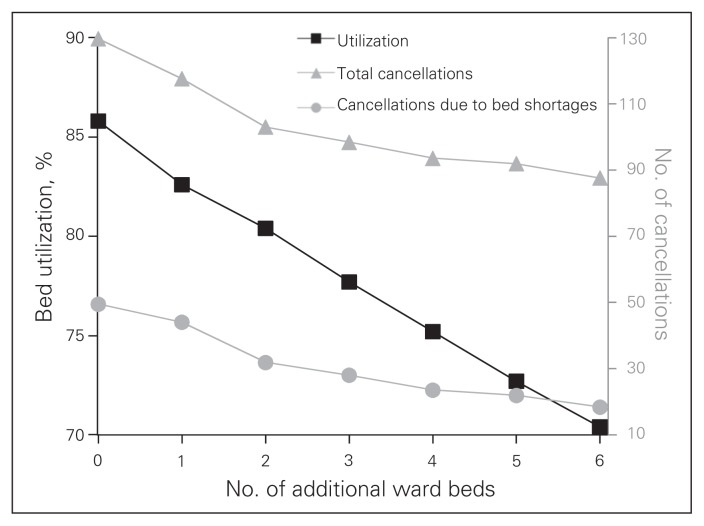
Methods: We used discrete event simulation modelling to represent perioperative processes at a hospital in Toronto, Canada. We tested the effects of the following 3 scenarios on the number of surgical cancellations: scheduling surgeons' operating days based on their patients' average length of stay in hospital, sequencing surgical procedures by average duration and variance, and increasing the number of postsurgical ward beds.
Results: The number of elective cancellations was reduced by scheduling surgeons whose patients had shorter average lengths of stay in hospital earlier in the week, sequencing shorter surgeries and those with less variance in duration earlier in the day, and by adding up to 2 additional beds to the postsurgical ward.
Conclusion: Discrete event simulation modelling can be used to develop strategies for improving efficiency in operating rooms.
Contexte: Dans les hôpitaux canadiens, qui sont généralement financés par des budgets annuels globaux, la surutilisation des blocs opératoires comporte un risque financier qui est souvent géré par l’annulation des interventions chirurgicales non urgentes. On ignore comment les différentes règles de préparation des calendriers affectent le taux d’annulation des chirurgies non urgentes.
Méthodes: Nous avons utilisé un modèle de simulation d’événements discrets pour représenter les marches à suivre périopératoires dans un hôpital de Toronto, au Canada. Nous avons vérifié les effets des 3 scénarios suivants sur le nombre de chirurgies annulées : préparation du calendrier des chirurgiens selon la durée moyenne de l’hospitalisation de leurs patients, enchaînement des interventions chirurgicales selon leur durée moyenne et la variabilité de leur durée et augmentation du nombre de lits dans les unités postopératoires.
Résultats: Le nombre de chirurgies non urgentes annulées a diminué lorsqu’on a planifié les interventions des chirurgiens dont les patients séjournaient moins longtemps à l’hôpital plus tôt au cours de la semaine, lorsqu’on a programmé les chirurgies plus brèves et les chirurgies à durée moins variable plus tôt au cours de la journée et lorsqu’on a ajouté 2 lits supplémentaires à l’unité postopératoire.
Conclusion: Les modèles de simulation d’événements discrets peuvent servir à développer des stratégies pour améliorer l’efficience des blocs opératoires.
References
-
- Healthcare Financial Management Association. Achieving operating room efficiency through process integration. Healthc Financ Manag. 2003;57 suppl 1-7 following 112. - PubMed
-
- Denton BT, Rahman AS, Nelson H, et al. Simulation of a multiple operating room surgical suite. Proceedings of the winter simulation conference, 2006; 2006 Dec. 3–6; Monterey (CA). New Jersey: IEEE; 2006. pp. 414–24.
-
- Marjamaa R, Vakkuri A, Kirvela O. Operating room management: Why, how and by whom? Acta Anaesthesiol Scand. 2008;52:596–600. - PubMed
-
- Glouberman S, Mintzberg H. Managing the care of health and the cure of disease part I: differentiation. Health Care Manage Rev. 2001;26:56–69. - PubMed
-
- Harper PR. A framework for operational modelling of hospital resources. Health Care Manag Sci. 2002;5:165–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources