

Withholding or continuing beta-blocker treatment before dipyridamole myocardial perfusion imaging for the diagnosis of coronary artery disease? A randomized clinical trial
- PMID: 23351617
- PMCID: PMC3565929
- DOI: 10.1186/2008-2231-21-8
Withholding or continuing beta-blocker treatment before dipyridamole myocardial perfusion imaging for the diagnosis of coronary artery disease? A randomized clinical trial
Abstract
Background: Although it has been shown that acute beta-blocker administration may reduce the presence or severity of myocardial perfusion defects with dipyridamole stress, little information is available about the potential effect of chronic beta-blocker treatment on the sensitivity of dipyridamole myocardial perfusion imaging (DMPI).
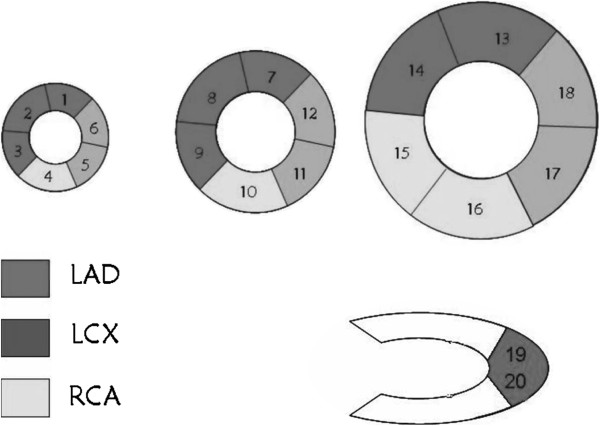
Methods: As a randomized clinical trial, one hundred twenty patients (103 male and 17 female) with angiographically confirmed CAD who were on long-term beta blocker therapy (≥3 months) enrolled in a randomized clinical trial study. The patients were allocated into two groups: Group A (n=60) in whom the beta-blocker agent was discontinued for 72h before DMPI and Group B (n=60) without discontinuation of beta-blockers prior to DMPI.
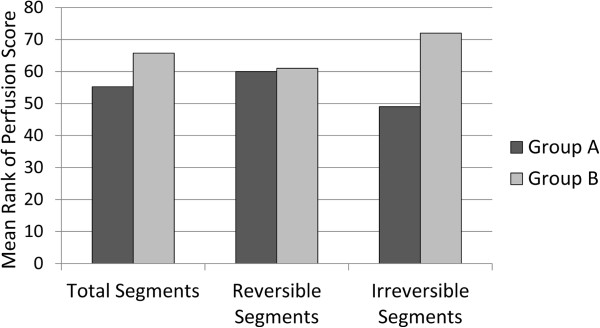
Results: No significant difference was noted between the groups concerning age, sex, type of the injected radiotracer and number of involved coronary vessels. The mean rank of total perfusion scores for whole myocardium (irrespective of reversibility or irreversibility) in group B was not significantly different from that of group A, (65.75 vs. 55.25, P=0.096). Regarding the only irreversible perfusion defects, the mean rank of perfusion score in group B was higher than that of group A for whole myocardium (72 vs. 49, P=0.0001); however, no difference was noted between two groups for only reversible perfusion defects (61.0 vs. 60.0, P=0.898). The overall sensitivity of DMPI for the diagnosis of CAD in group A (91.7%) was not statistically different from group B (90%).
Conclusion: Beta-blocker withholding before DMPI did not generally affect the sensitivity of the test for the diagnostic purposes in our study. Thus, beta-blocker withdrawal for just the purpose of diagnostic imaging is not mandatory particularly when medication discontinuation may cause the patients to face increased risk of heart events.
Figures
References
-
- Cuocolo A, Petretta M, Acampa W, De Falco T. Gated SPECT myocardial perfusion imaging: the further improvements of an excellent tool. Q J Nucl Med Mol Imaging. 2010;54(2):129–144. - PubMed
-
- Fallahi B, Beiki D, Gholamrezanezhad A, Mahmoudian B, Ansari Gilani K, Eftekhari M, Fard-Esfahani A, Mohseni Z, Saghari M. Single 99mTc Sestamibi injection, double acquisition gated SPECT after stress and during low-dose dobutamine infusion: a new suggested protocol for evaluation of myocardial perfusion. Int J Cardiovasc Imaging. 2008;24(8):825–835. doi: 10.1007/s10554-008-9328-y. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
