

Treatment outcomes in REM sleep behavior disorder
- PMID: 23352028
- PMCID: PMC3617579
- DOI: 10.1016/j.sleep.2012.09.018
Treatment outcomes in REM sleep behavior disorder
Abstract
Objective: REM sleep behavior disorder (RBD) is usually characterized by potentially injurious dream enactment behaviors (DEB). RBD treatment aims to reduce DEBs and prevent injury, but outcomes require further elucidation. We surveyed RBD patients to describe longitudinal treatment outcomes with melatonin and clonazepam.
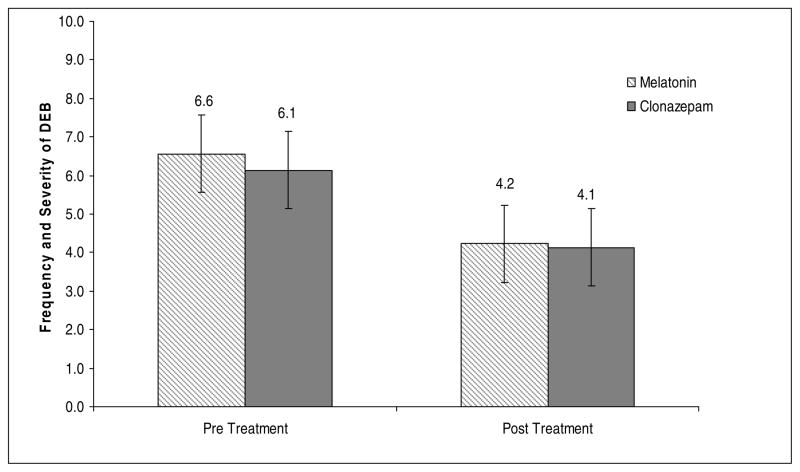
Methods: We surveyed and reviewed records of consecutive RBD patients seen at Mayo Clinic between 2008-2010 to describe RBD-related injury frequency-severity as well as RBD visual analog scale (VAS) ratings, medication dosage, and side effects. Statistical analyses were performed with appropriate non-parametric matched pairs tests before and after treatment, and with comparative group analyses for continuous and categorical variables between treatment groups. The primary outcome variables were RBD VAS ratings and injury frequency.
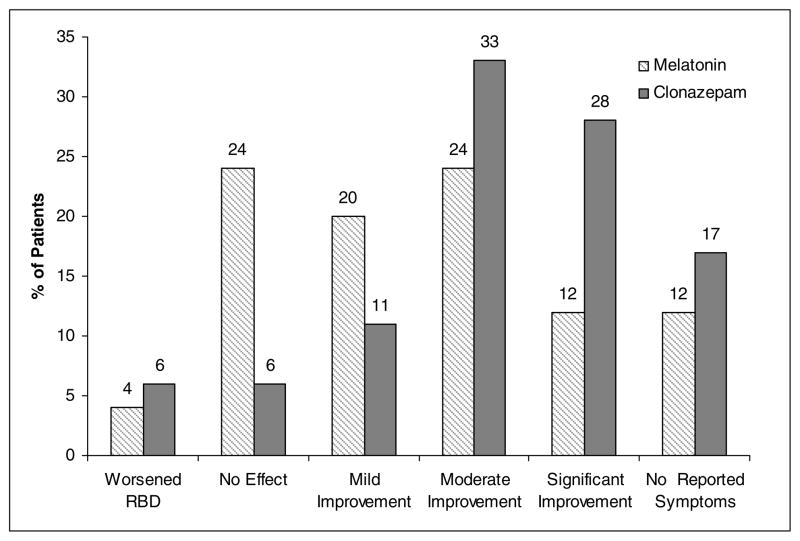
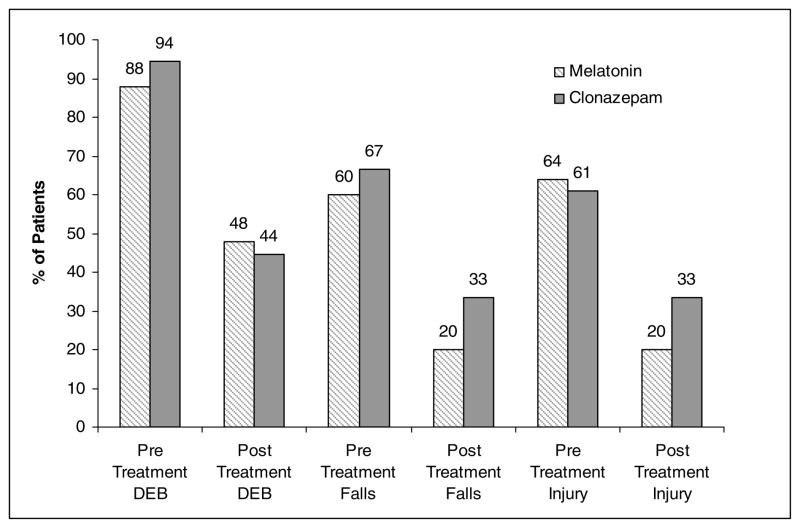
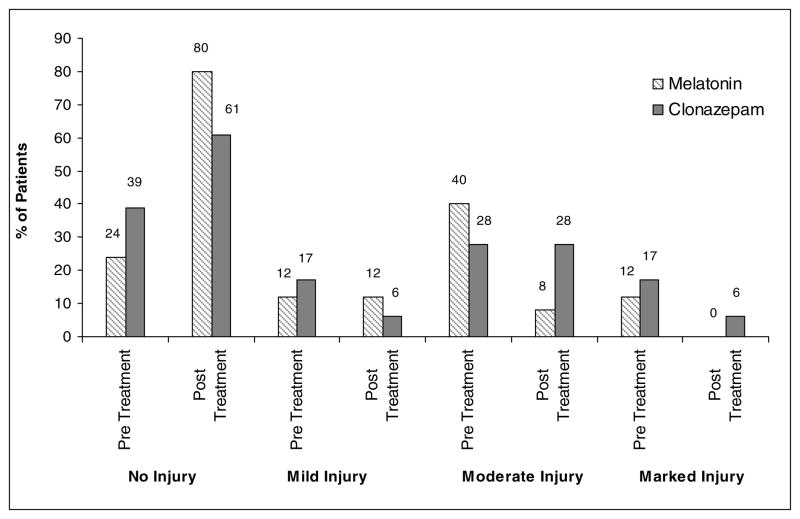
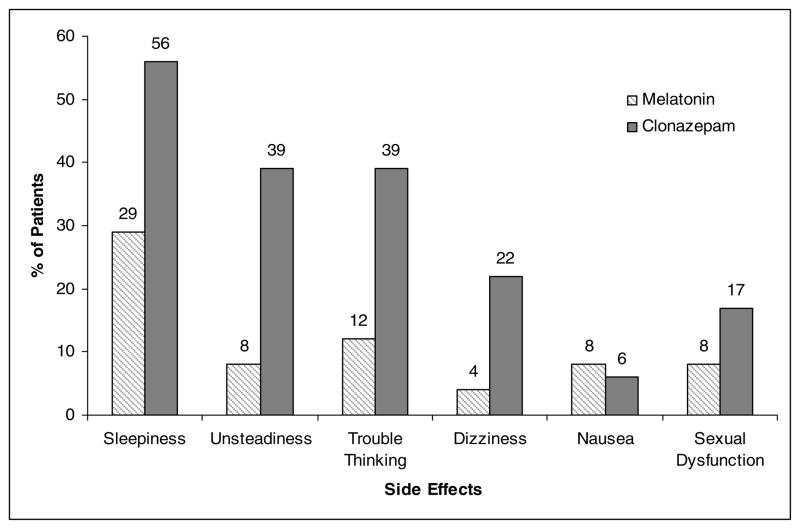
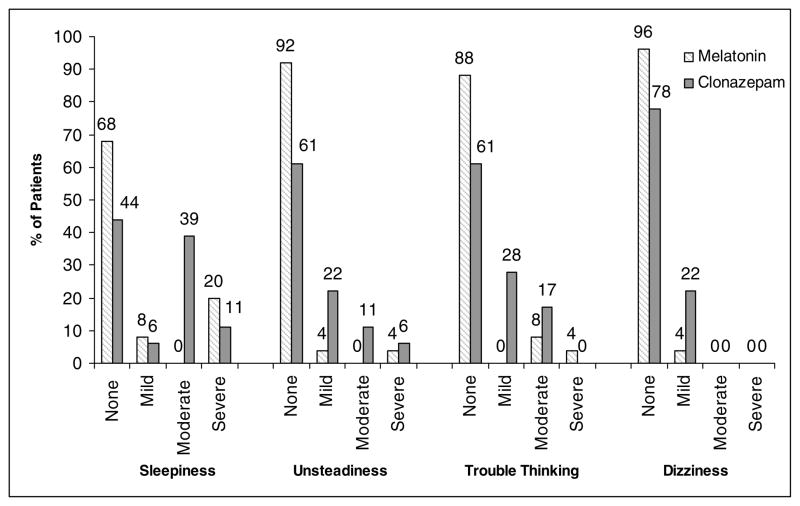
Results: Forty-five (84.9%) of 53 respondent surveys were analyzed. Mean age was 65.8 years and 35 (77.8%) patients were men. Neurodegenerative disorders were seen in 24 (53%) patients and 25 (56%) received antidepressants. Twenty-five patients received melatonin, 18 received clonazepam, and two received both as initial treatment. Before treatment, 27 patients (60%) reported an RBD associated injury. Median dosages were melatonin 6 mg and clonazepam 0.5 mg. RBD VAS ratings were significantly improved following both treatments (p(m) = 0.0001, p(c) = 0.0005). Melatonin-treated patients reported significantly reduced injuries (p(m) = 0.001, p(c) = 0.06) and fewer adverse effects (p = 0.07). Mean durations of treatment were no different between groups (for clonazepam 53.9 ± 29.5 months, and for melatonin 27.4 ± 24 months, p = 0.13) and there were no differences in treatment retention, with 28% of melatonin and 22% of clonazepam-treated patients discontinuing treatment (p = 0.43).
Conclusions: Melatonin and clonazepam were each reported to reduce RBD behaviors and injuries and appeared comparably effective in our naturalistic practice experience. Melatonin-treated patients reported less frequent adverse effects than those treated with clonazepam. More effective treatments that would eliminate injury potential and evidence-based treatment outcomes from prospective clinical trials for RBD are needed.
Copyright © 2012 Elsevier B.V. All rights reserved.
Figures
References
-
- American Academy of Sleep Medicine. Diagnositc and coding manual. 2. American Academy of Sleep Medicine; 2005. International classification of sleep disorders.
-
- Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9(2):293–308. - PubMed
-
- Iranzo A, Santamaria J, Tolosa E. The clinical and pathophysiological relevance of REM sleep behavior disorder in neurodegenerative diseases. Sleep Med Rev. 2009;13(6):385–40. - PubMed
-
- Olson EJ, Boeve BF, Silber MH. Rapid eye movement sleep behaviour disorder: demographic, clinical and laboratory findings in 93 cases. Brain: J Neurol. 2000;123(Pt 2):331–9. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
