

MRI predicts ALVAL and tissue damage in metal-on-metal hip arthroplasty
- PMID: 23354460
- PMCID: PMC3890156
- DOI: 10.1007/s11999-013-2788-y
MRI predicts ALVAL and tissue damage in metal-on-metal hip arthroplasty
Abstract
Background: Adverse local tissue reactions (ALTR) around metal-on-metal (MOM) hip arthroplasties are increasingly being recognized as a cause of failure. These reactions may be associated with intraoperative tissue damage and complication rates as high as 50% after revision. Although MRI can identify ALTR in MOM hips, it is unclear whether the MRI findings predict those at revision surgery.
Questions/purposes: We therefore (1) identified which MRI characteristics correlated with histologically confirmed ALTR (using the aseptic lymphocytic vasculitis-associated lesions [ALVAL] score) and intraoperative tissue damage and (2) developed a predictive model using modified MRI to detect ALVAL and quantify intraoperative tissue damage.
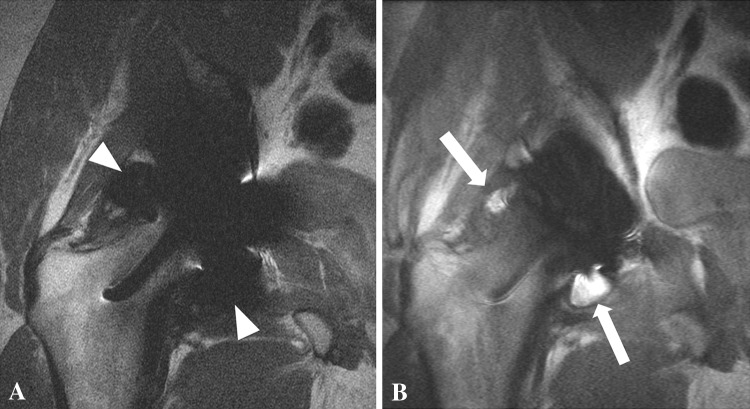
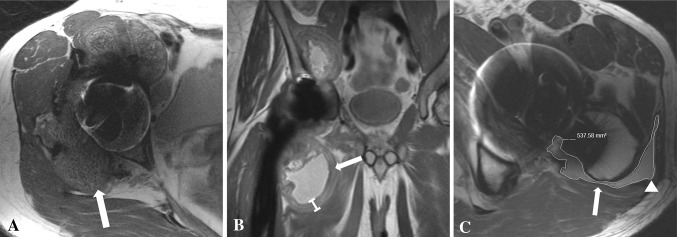
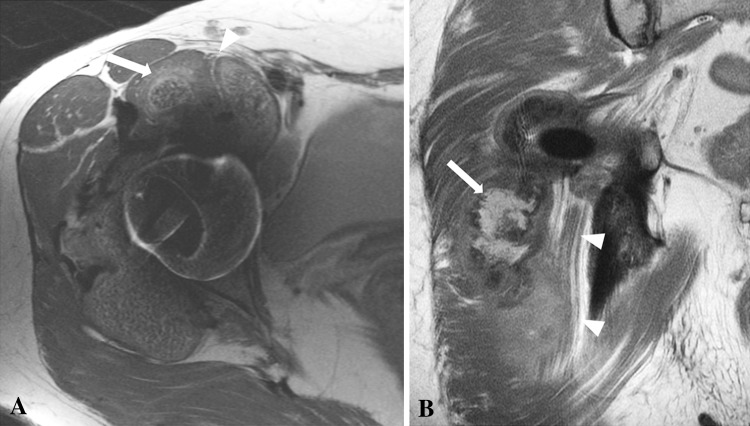
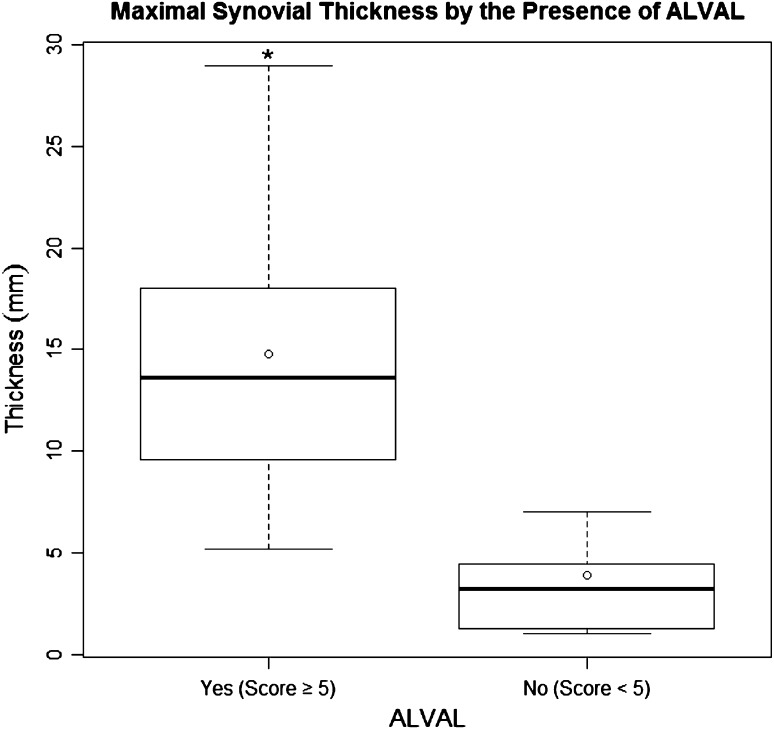
Methods: We retrospectively reviewed 68 patients with failed MOM hip arthroplasties who underwent preoperative MRI and subsequent revision surgery. Images were analyzed to determine synovial volume, osteolysis, and synovial thickness. The ALVAL score was used to grade tissue samples, thus identifying a subset of patients with ALTR. Intraoperative tissue damage was graded using a four-point scale. Random forest analysis determined the sensitivity and specificity of MRI characteristics in detecting ALVAL (score ≥ 5) and intraoperative tissue damage.
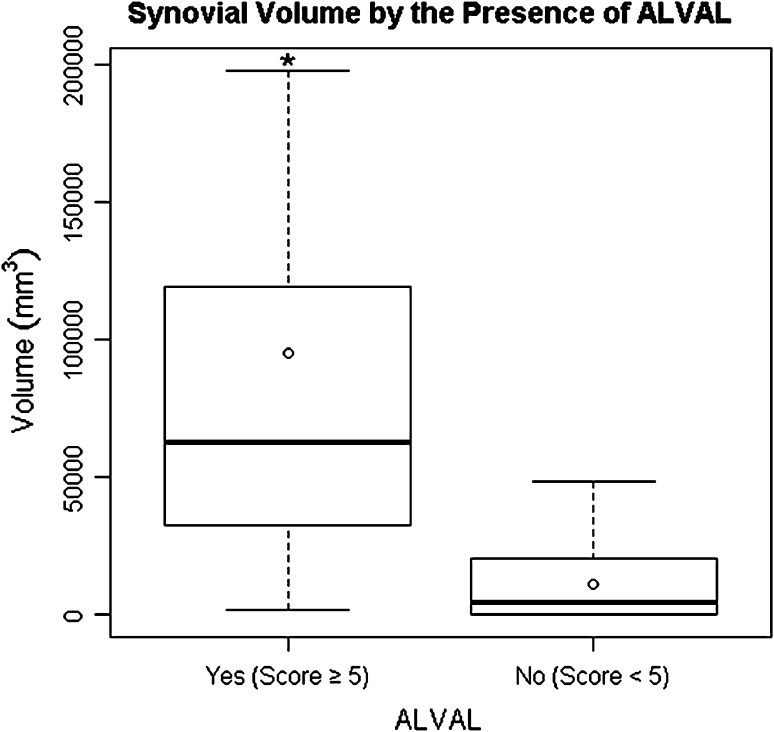
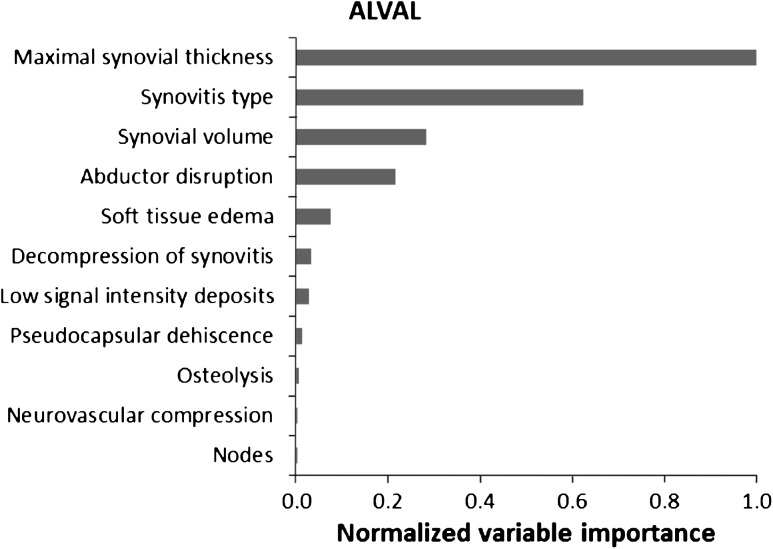
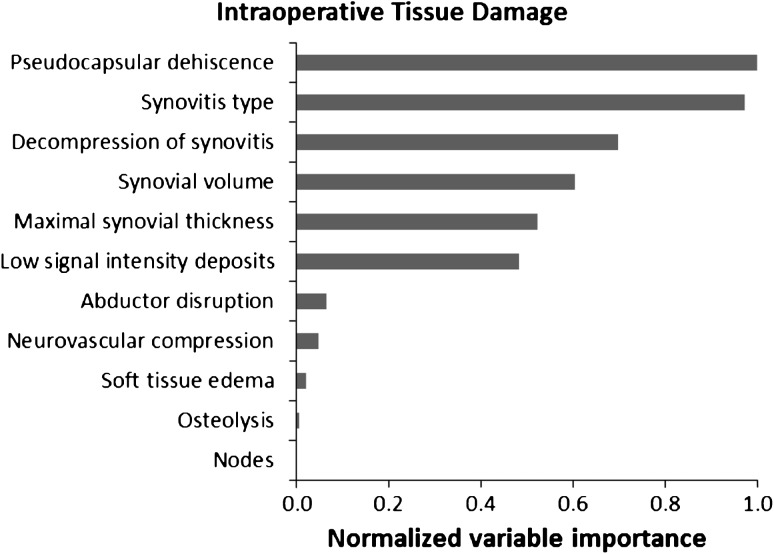
Results: Maximal synovial thicknesses and synovial volumes as determined on MRI correlated with the ALVAL score and were higher in cases of severe intraoperative tissue damage. Our MRI predictive model showed sensitivity and specificity of 94% and 87%, respectively, for detecting ALVAL and 90% and 86%, respectively, for quantifying intraoperative tissue damage.
Conclusions: MRI is sensitive and specific in detecting ALVAL and tissue damage in patients with MOM hip implants. MRI can be used as a screening tool to guide surgeons toward timely revision surgery.
Figures


References
-
- Dorr LD, Wan Z, Longjohn DB, Dubois B, Murken R. Total hip arthroplasty with use of the Metasul metal-on-metal articulation: four to seven-year results. J Bone Joint Surg Am. 2000;82:789–798. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
