

Impingement adversely affects 10-year survivorship after periacetabular osteotomy for DDH
- PMID: 23354462
- PMCID: PMC3613512
- DOI: 10.1007/s11999-013-2799-8
Impingement adversely affects 10-year survivorship after periacetabular osteotomy for DDH
Abstract
Background: Although periacetabular osteotomy (PAO) for developmental dysplasia of the hip (DDH) provides conceptual advantages compared with other osteotomies and reportedly is associated with joint survivorship of 60% at 20 years, the beneficial effect of proper acetabular reorientation with concomitant arthrotomy and creation of femoral head-neck offset on 10-year hip survivorship remains unclear.
Questions/purposes: We asked the following questions: (1) Does the 10-year survivorship of the hip after PAO improve with proper acetabular reorientation and a spherical femoral head; (2) does the Merle d'Aubigné-Postel score improve; (3) can the progression of osteoarthritis (OA) be slowed; and (4) what factors predict conversion to THA, progression of OA, or a Merle d'Aubigné-Postel score less than 15 points?
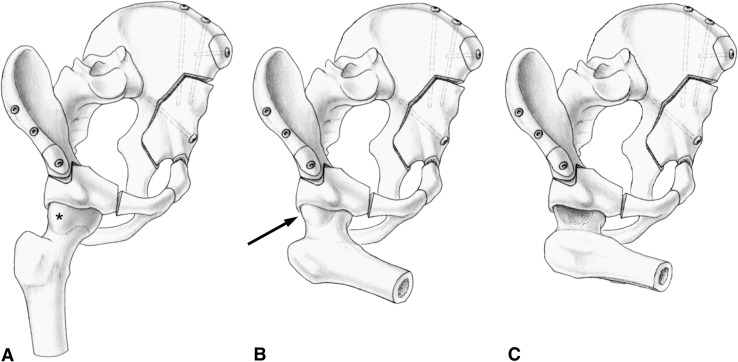
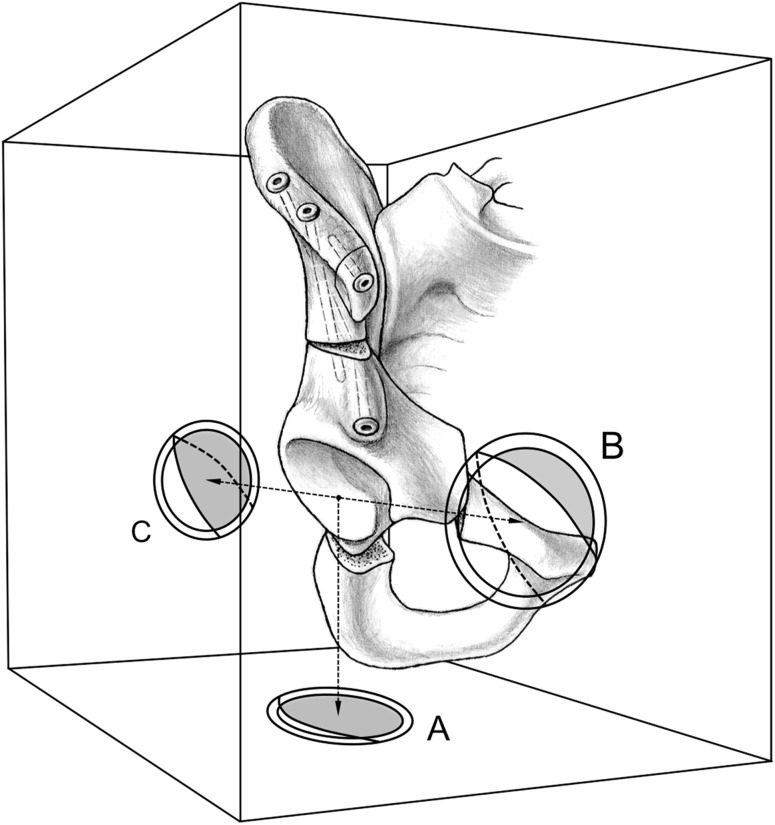
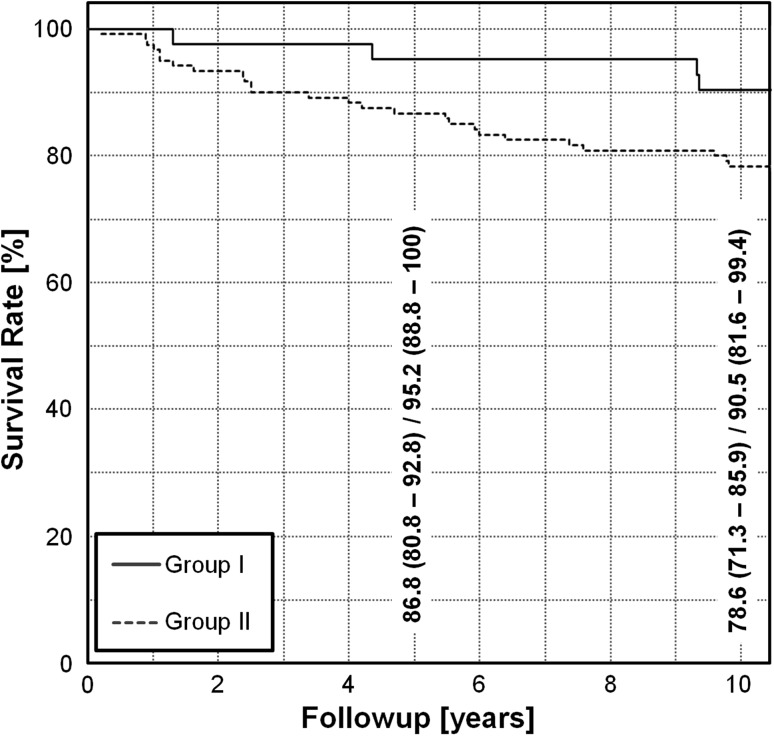
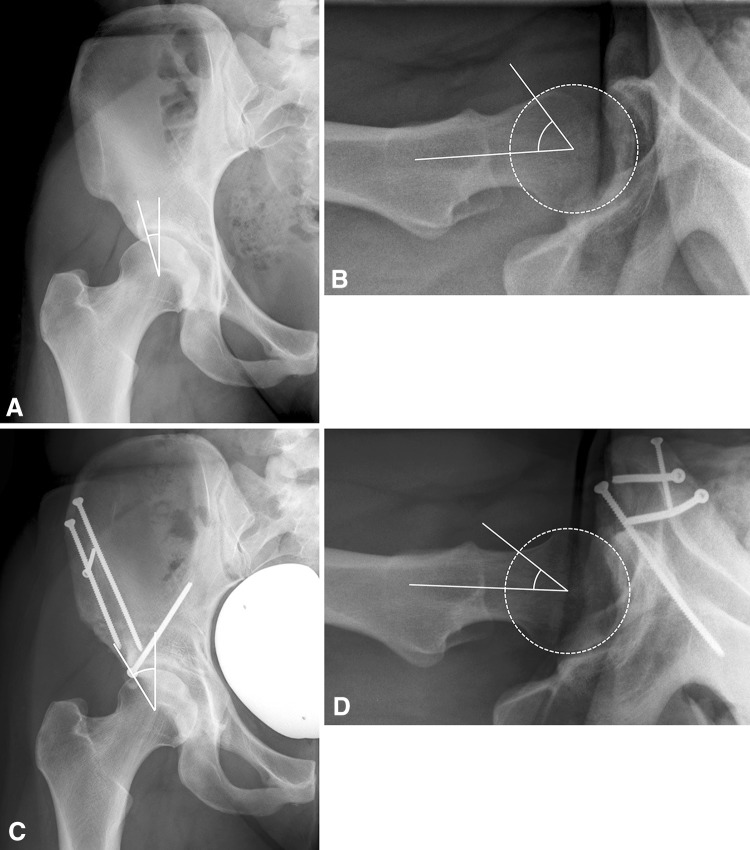
Methods: We retrospectively reviewed 147 patients who underwent 165 PAOs for DDH with two matched groups: Group I (proper reorientation and spherical femoral head) and Group II (improper reorientation and aspherical femoral head). We compared the Kaplan-Meier survivorship, Merle d'Aubigné-Postel scores, and progression of OA in both groups. A Cox regression analysis (end points: THA, OA progression, or Merle d'Aubigné-Postel score less than 15) was performed to detect factors predicting failure. The minimum followup was 10 years (median, 11 years; range, 10-14 years).
Results: An increased survivorship was found in Group I. The Merle d'Aubigné-Postel score did not differ. Progression of OA in Group I was slower than in Group II. Factors predicting failure included greater age, lower preoperative Merle d'Aubigné-Postel score, and the presence of a Trendelenburg sign, aspherical head, OA, subluxation, postoperative acetabular retroversion, excessive acetabular anteversion, and undercoverage.
Conclusions: Proper acetabular reorientation and the creation of a spherical femoral head improve long-term survivorship and decelerate OA progression in patients with DDH.
Figures

References
-
- Apley AG, Wientroub S. The sagging rope sign in Perthes’ disease and allied disorders. J Bone Joint Surg Br. 1981;63:43–47. - PubMed
-
- Cox DR. Regression models and life-tables. J Roy Stat Soc B. 1972;34:187–191.
-
- D’Aubigne RM, Postel M. Functional results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg Am. 1954;36:451–475. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
