

Effect of oral digoxin in high-risk heart failure patients: a pre-specified subgroup analysis of the DIG trial
- PMID: 23355060
- PMCID: PMC3707428
- DOI: 10.1093/eurjhf/hft010
Effect of oral digoxin in high-risk heart failure patients: a pre-specified subgroup analysis of the DIG trial
Abstract
Aims: In the Digitalis Investigation Group (DIG) trial, digoxin reduced mortality or hospitalization due to heart failure (HF) in several pre-specified high-risk subgroups of HF patients, but data on protocol-specified 2-year outcomes were not presented. In the current study, we examined the effect of digoxin on HF death or HF hospitalization and all-cause death or all-cause hospitalization in high-risk subgroups during the protocol-specified 2 years of post-randomization follow-up.
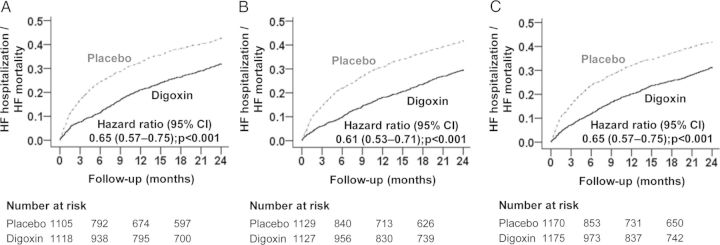
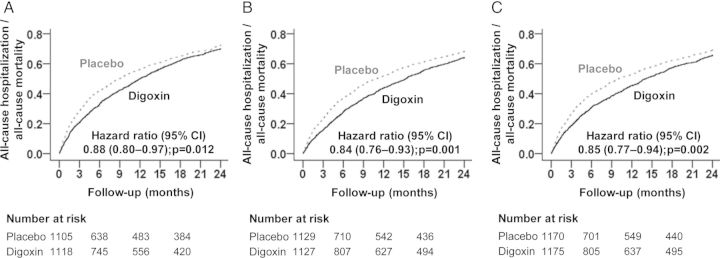
Methods and results: In the DIG trial, 6800 ambulatory patients with chronic HF, normal sinus rhythm, and LVEF ≤45% (mean age 64 years, 26% women, 17% non-whites) were randomized to receive digoxin or placebo. The three high-risk groups were defined as NYHA class III-IV symptoms (n = 2223), LVEF <25% (n = 2256), and cardiothoracic ratio (CTR) >55% (n = 2345). In all three high-risk subgroups, compared with patients in the placebo group, those in the digoxin group had a significant reduction in the risk of the 2-year composite endpoint of HF mortality or HF hospitalization: NYHA III-IV [hazard ratio (HR) 0.65; 95% confidence interval (CI) 0.57-0.75; P < 0.001], LVEF <25% (HR 0.61; 95% CI 0.53-0.71; P < 0.001), and CTR >55% (HR 0.65; 95% CI 0.57-0.75; P < 0.001). Digoxin-associated HRs (95% CI) for 2-year all-cause mortality or all-cause hospitalization for subgroups with NYHA III-IV, LVEF <25%, and CTR >55% were 0.88 (0.80-0.97; P = 0.012), 0.84 (0.76-0.93; P = 0.001), and 0.85 (0.77-0.94; P = 0.002), respectively.
Conclusions: Digoxin improves outcomes in chronic HF patients with NYHA class III-IV, LVEF <25%, or CTR >55%, and should be considered in these patients.
Figures
References
-
- The Digitalis Investigation Group Investigators. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–533. - PubMed
-
- Uretsky BF, Young JB, Shahidi FE, Yellen LG, Harrison MC, Jolly MK. Randomized study assessing the effect of digoxin withdrawal in patients with mild to moderate chronic congestive heart failure: results of the PROVED trial. PROVED Investigative Group. J Am Coll Cardiol. 1993;22:955–962. - PubMed
-
- Packer M, Gheorghiade M, Young JB, Costantini PJ, Adams KF, Cody RJ, Smith LK, Van Voorhees L, Gourley LA, Jolly MK. Withdrawal of digoxin from patients with chronic heart failure treated with angiotensin-converting-enzyme inhibitors. RADIANCE Study. N Engl J Med. 1993;329:1–7. - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Køber L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Rnnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Bax JJ, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Kirchhof P, Knuuti J, Kolh P, McDonagh T, Moulin C, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Torbicki A, Vahanian A, Windecker S, McDonagh T, Sechtem U, Bonet LA, Avraamides P, Ben Lamin HA, Brignole M, Coca A, Cowburn P, Dargie H, Elliott P, Flachskampf FA, Guida GF, Hardman S, Iung B, Merkely B, Mueller C, Nanas JN, Nielsen OW, Orn S, Parissis JT, Ponikowski P; ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14:803–869. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391–e479. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
