

Overdiagnosis among women attending a population-based mammography screening program
- PMID: 23355313
- PMCID: PMC3708102
- DOI: 10.1002/ijc.28052
Overdiagnosis among women attending a population-based mammography screening program
Abstract
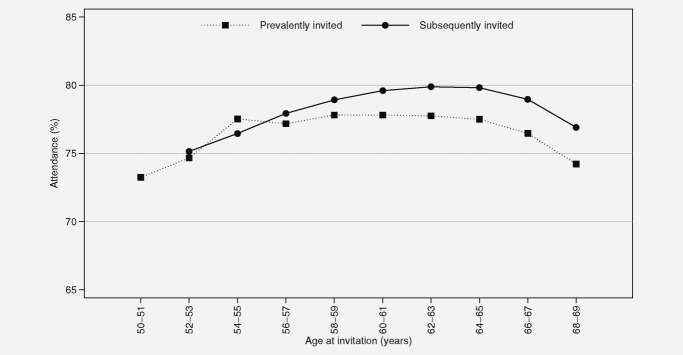
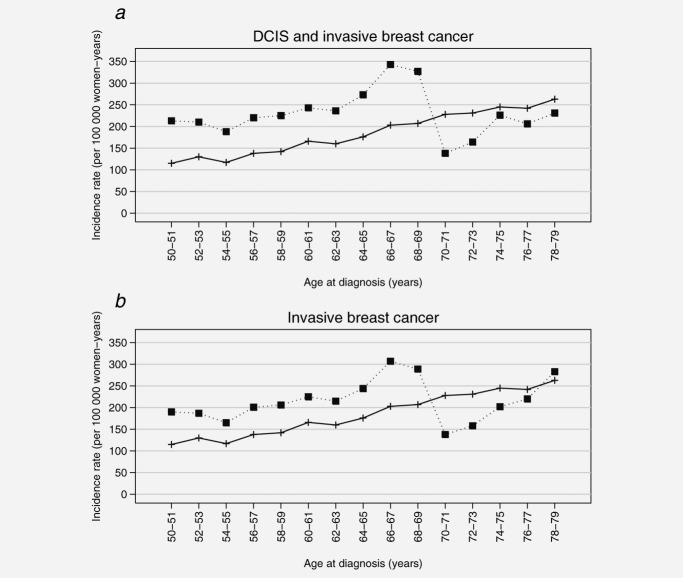
Increased incidence of ductal carcinoma in situ (DCIS) and invasive breast cancer (IBC) after introduction of organized screening has prompted debate about overdiagnosis. The aim was to examine the excess in incidence of DCIS and IBC during the screening period and the deficit after women left the program, and thereby to estimate the proportion of overdiagnosis. Women invited to the Norwegian Breast Cancer Screening Program were analyzed for DCIS or IBC during the period 1995-2009. Incidence rate ratios (IRRs) were calculated for attended vs. never attended women. The IRRs were adjusted by Mantel-Haenszel (MH) method and applied to a set of reference rates and a reference population to estimate the proportion of overdiagnosis during the women's lifespan after the age of 50 years. A total of 702,131 women were invited to the program. An excess of DCIS and IBC was observed among women who attended screening during the screening period; prevalently invited women aged 50-51 years had a MH IRR of 1.86 (95% CI 1.65-2.09) and subsequently invited women aged 52-69 years had a MH IRR of 1.56 (95% CI 1.45-1.68). In women aged 70-79 years, a deficit of 30% (MH IRR 0.70, 95% CI 0.62-0.80) was observed 1-10 years after they left the screening program. The estimated proportion of overdiagnosis varied from 10 to 20% depending on outcome and whether the women were invited or actually screened. The results highlight the need for individual data with longitudinal screening history and long-term follow-up as a basis for estimating overdiagnosis.
Copyright © 2013 UICC.
Figures
Comment in
-
Failure to account for selection-bias.Int J Cancer. 2013 Dec 1;133(11):2751-3. doi: 10.1002/ijc.28244. Epub 2013 Jun 17. Int J Cancer. 2013. PMID: 23649899 No abstract available.
-
Response to comments by Kalager et al. and Zahl et al.Int J Cancer. 2013 Dec 1;133(11):2756-7. doi: 10.1002/ijc.28247. Epub 2013 May 29. Int J Cancer. 2013. PMID: 23650012 No abstract available.
-
Overdiagnosis of breast cancer in Norway: what have the authors adjusted for?Int J Cancer. 2013 Dec 1;133(11):2754-5. doi: 10.1002/ijc.28248. Epub 2013 May 29. Int J Cancer. 2013. PMID: 23650050 No abstract available.
References
-
- Glass AG, Lacey JV, Jr, Carreon JD, et al. Breast cancer incidence, 1980–2006: combined roles of menopausal hormone therapy, screening mammography, and estrogen receptor status. J Natl Cancer Inst. 2007;99:1152–61. - PubMed
-
- Sorum R, Hofvind S, Skaane P, et al. Trends in incidence of ductal carcinoma in situ: the effect of a population-based screening programme. Breast. 2010;19:499–505. - PubMed
-
- Vainio H, Bianchini F, editors. IARC handbooks of cancer prevention. Breast cancer screening. Vol. 7. Lyon: IARC Press; 2002. p. 229.
-
- Kalager M, Adami HO, Bretthauer M, et al. Overdiagnosis of invasive breast cancer due to mammography screening: results from the Norwegian screening program. Ann Intern Med. 2012;156:491–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
