

Juvenile systemic lupus erythematosus with primary neuropsychiatric presentation
- PMID: 23355592
- PMCID: PMC3603605
- DOI: 10.1136/bcr-2012-008270
Juvenile systemic lupus erythematosus with primary neuropsychiatric presentation
Abstract
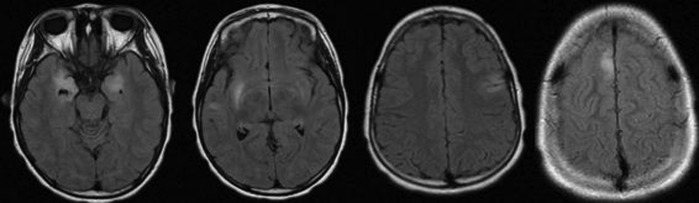
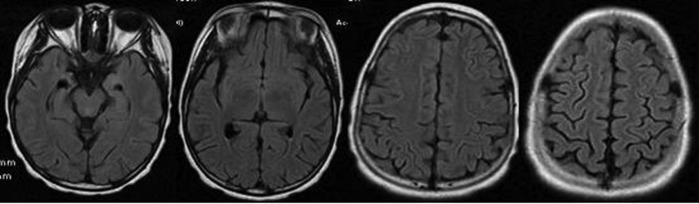
Systemic lupus erythematosus (SLE) is an autoimmune disease with multiple manifestations in several organs and systems. Neuropsychiatric manifestations can occur in 22-95% of paediatric cases, being much less frequent as an initial clinical event. We report a case of SLE, presenting primarily with neuropsychiatric symptoms. An African-descendant 7-year-old girl was admitted with a 4-day history of ataxia, diplopia and morning vomiting, as well as severe headache, psychiatric symptoms and cognitive dysfunction beginning 1 year prior to admission. Brain MRI was suggestive of encephalitis. Investigation excluded infectious aetiology. Immunological markers revealed high titre of antinuclear and anti-double-stranded DNA antibodies. Neuropsychiatric lupus (NPL) was considered, and cyclophosphamide and methylprednisolone pulses were started, with good initial response. Clinical deterioration motivated therapy with azathioprine with subsequent clinical stabilisation and a latent cognitive dysfunction. In unusual encephalitis presentation, a wide range of differential diagnosis has to be considered. Primary NPL presents difficult diagnostic and therapeutic challenges.
Figures
References
-
- Harel L, Sandborg C, Lee T, et al. Neuropsychiatric manifestations in pediatric systemic lupus erythematosus and association with antiphospholipid antibodies. J Rheumatol 2006;33:1873–7 - PubMed
-
- Sibbitt WL, Jr, Brandt JR, Johnson CR, et al. The incidence and prevalence of neuropsychiatric syndromes in pediatric onset systemic lupus erythematosus. J Rheumatol 2002;29:1536–42 - PubMed
-
- Yu HH, Lee JH, Wang LC, et al. Neuropsychiatric manifestations in pediatric systemic lupus erythematosus: a 20-year study. Lupus 2006;15:651–7 - PubMed
-
- Benseler SM, Silverman ED. Neuropsychiatric involvement in pediatric systemic lupus erythematosus. Lupus 2007;16:564–71 - PubMed
-
- Hiraki LT, Benseler SM, Tyrrell PN, et al. Clinical and laboratory characteristics and long-term outcomes of pediatric systemic lupus erythematosus: a longitudinal study. J Pediatr 2008;152:550–6 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical