

Variation exists in rates of admission to intensive care units for heart failure patients across hospitals in the United States
- PMID: 23355624
- PMCID: PMC3688061
- DOI: 10.1161/CIRCULATIONAHA.112.001088
Variation exists in rates of admission to intensive care units for heart failure patients across hospitals in the United States
Abstract
Background: Despite increasing attention on reducing relatively costly hospital practices while maintaining the quality of care, few studies have examined how hospitals use the intensive care unit (ICU), a high-cost setting, for patients admitted with heart failure (HF). We characterized hospital patterns of ICU admission for patients with HF and determined their association with the use of ICU-level therapies and patient outcomes.
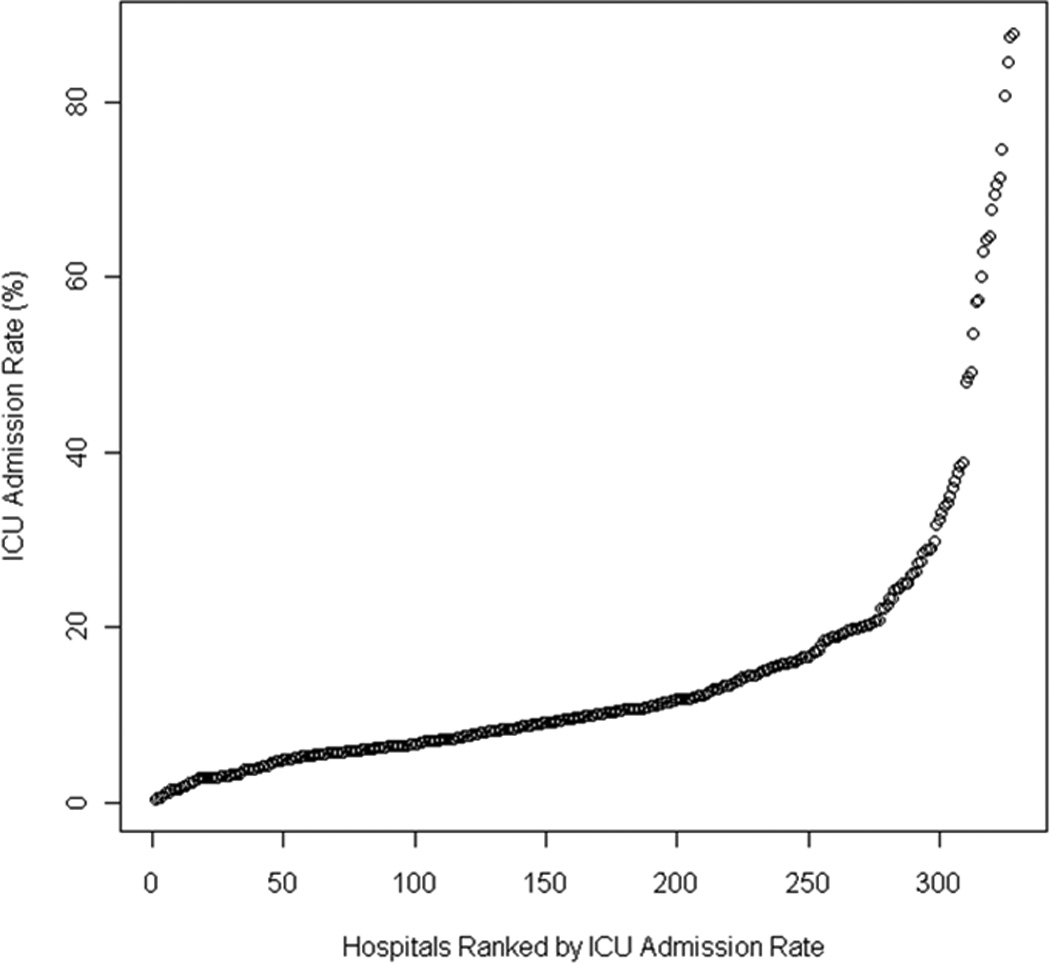
Methods and results: We identified 166 224 HF discharges from 341 hospitals in the 2009-2010 Premier Perspective database. We excluded hospitals with <25 HF admissions, patients <18 years old, and transfers. We defined ICU as including medical ICU, coronary ICU, and surgical ICU. We calculated the percent of patients admitted directly to an ICU. We compared hospitals in the top quartile (high ICU admission) with the remaining quartiles. The median percentage of ICU admission was 10% (interquartile range, 6%-16%; range, 0%-88%). In top-quartile hospitals, treatments requiring an ICU were used less often; the percentage of ICU days receiving mechanical ventilation was 6% for the top quartile versus 15% for the others; noninvasive positive pressure ventilation, 8% versus 19%; vasopressors and/or inotropes, 9% versus 16%; vasodilators, 6% versus 12%; and any of these interventions, 26% versus 51%. Overall HF in-hospital risk-standardized mortality was similar (3.4% versus 3.5%; P=0.2).
Conclusions: ICU admission rates for HF varied markedly across hospitals and lacked association with in-hospital risk-standardized mortality. Greater ICU use correlated with fewer patients receiving ICU interventions. Judicious ICU use could reduce resource consumption without diminishing patient outcomes.
Conflict of interest statement
Figures
References
-
- Adams KF, Jr, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, Berkowitz RL, Galvao M, Horton DP. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE) Am Heart J. 2005;149:209–216. - PubMed
-
- Chalfin DB. Cost-effectiveness analysis in health care. Hosp Cost Manag Account. 1995;7:1–8. - PubMed
-
- Halpern NA, Bettes L, Greenstein R. Federal and nationwide intensive care units and healthcare costs: 1986–1992. Crit Care Med. 1994;22:2001–2007. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update incorporated into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the International Society for Heart and Lung Transplantation. J Am Coll Cardiol. 2009;53:e1–e90. - PubMed
-
- Dlugacz YD, Stier L, Lustbader D, Jacobs MC, Hussain E, Greenwood A. Expanding a performance improvement initiative in critical care from hospital to system. Jt Comm J Qual Improv. 2002;28:419–434. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
