

Comparison of absolute serum creatinine changes versus Kidney Disease: Improving Global Outcomes consensus definitions for characterizing stages of acute kidney injury
- PMID: 23355628
- PMCID: PMC3685303
- DOI: 10.1093/ndt/gfs533
Comparison of absolute serum creatinine changes versus Kidney Disease: Improving Global Outcomes consensus definitions for characterizing stages of acute kidney injury
Abstract
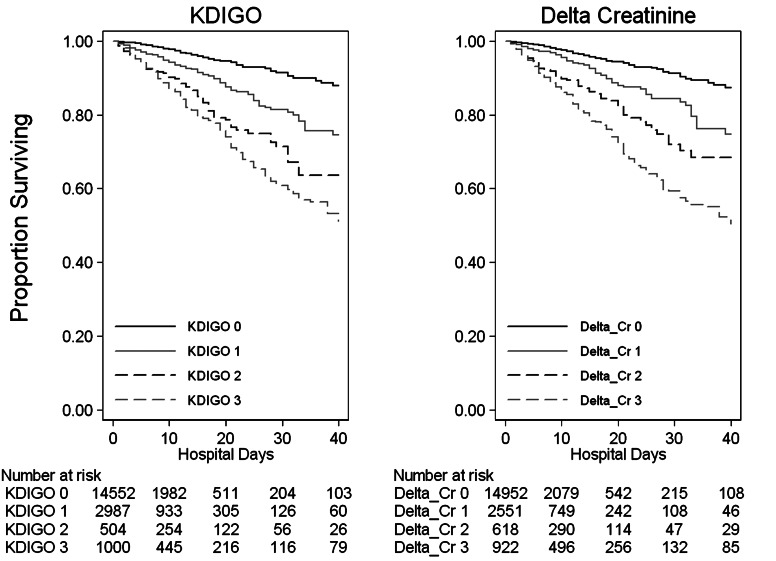
Background: The Kidney Disease: Improving Global Outcomes (KDIGO) system for classification of acute kidney injury (AKI) severity utilizes a staging schema based on relative changes in serum creatinine (sCr) concentration and urine output. This study compares the in-hospital mortality associated with KDIGO-defined AKI stages and AKI stages defined by absolute sCr increases ('Delta-Creatinine').
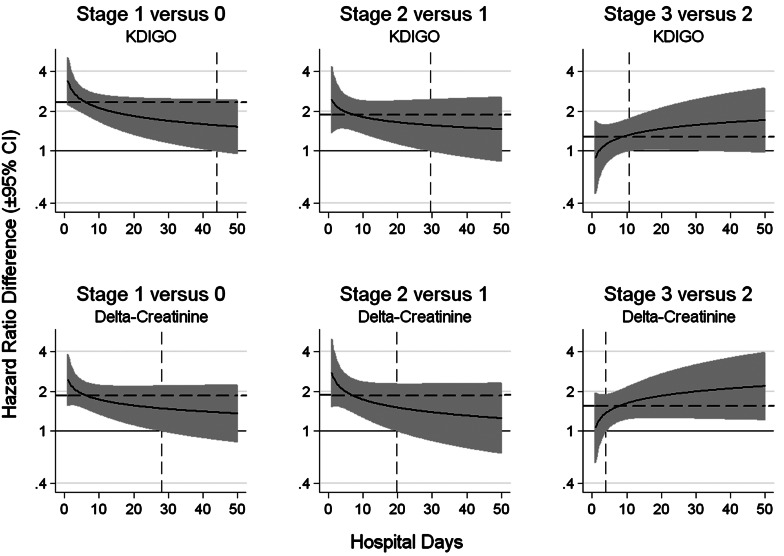
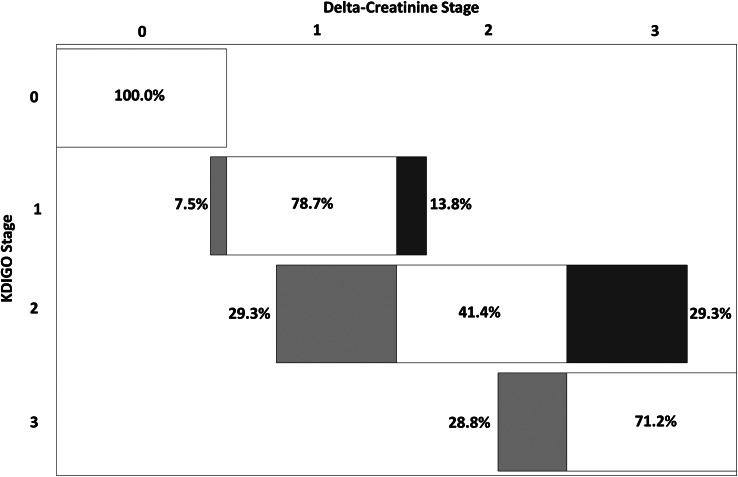
Methods: The study included an analysis of hospital discharge and laboratory data from an urban academic medical center over a 1-year period. Including adult in-patients undergoing two or more sCr measurements, the study classified AKI stages using the KDIGO consensus standards as well as absolute increases in sCr ('Delta-Creatinine'); Stage 0, sCr increase <0.3 mg/dL, Stage 1, sCr increase 0.3-0.69 mg/dL, Stage 2, sCr increase 0.7-1.19 mg/dL and Stage 3, sCr increase ≥1.2 mg/dL or initiation of renal replacement therapy. The Delta-Creatinine cut-points were defined to optimize discrimination of in-patient mortality between AKI stages. The associations between KDIGO and Delta-Creatinine AKI stages and in-hospital mortality were compared using the time-dependent hazard ratios (HRs) and the net reclassification improvement (NRI).
Results: Of the 19 878 hospitalizations included in the analysis, the prevalence of AKI was 23.4% as defined by the KDIGO criteria. The Delta-Creatinine system discriminated the differences between adjacent AKI stages (i.e. 1 versus 0, 2 versus 1, 3 versus 3) earlier than the KDIGO system. The NRI between Delta-Creatinine and KDIGO for the prediction of mortality was 9.7% [95% confidence interval (CI) 6.2-13.2%]. Stratification by age, sex, race and history of chronic kidney disease (CKD) resulted in similar NRI values.
Conclusion: The Delta-Creatinine system, based on the absolute increases in sCr, provides a promising alternative to the KDIGO system for characterizing the severity of AKI and its associations with in-patient mortality.
Keywords: acute kidney injury; chronic kidney disease; health services; hospital mortality.
Figures
Comment in
-
Defining AKI: closer to getting the math right.Nephrol Dial Transplant. 2013 Jun;28(6):1340-2. doi: 10.1093/ndt/gft011. Epub 2013 Mar 10. Nephrol Dial Transplant. 2013. PMID: 23479094 No abstract available.
References
-
- Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012;81:819–825. - PubMed
-
- Newsome BB, Warnock DG, McClellan WM, et al. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med. 2008;168:609–616. - PubMed
-
- Ricci Z, Cruz D, Ronco C. The RIFLE criteria and mortality in acute kidney injury: a systematic review. Kidney Int. 2008;73:538–546. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
