

Determinants of self-reported smoking and misclassification during pregnancy, and analysis of optimal cut-off points for urinary cotinine: a cross-sectional study
- PMID: 23355667
- PMCID: PMC3563144
- DOI: 10.1136/bmjopen-2012-002034
Determinants of self-reported smoking and misclassification during pregnancy, and analysis of optimal cut-off points for urinary cotinine: a cross-sectional study
Abstract
Objectives: To estimate the prevalence and factors associated with smoking and misclassification in pregnant women from INMA (INfancia y Medio Ambiente, Environment and Childhood) project, Spain, and to assess the optimal cut-offs for urinary cotinine (UC) that best distinguish daily and occasional smokers with varying levels of second-hand smoke (SHS) exposure.
Design: We used logistic regression models to study the relationship between sociodemographic variables and self-reported smoking and misclassification (self-reported non-smokers with UC >50 ng/ml). Receiver operating characteristic (ROC) curves were used to calculate the optimal cut-off point for discriminating smokers. The cut-offs were also calculated after stratification among non-smokers by the number of sources of SHS exposure. The cut-off points used to discriminate smoking status were the level of UC given by Youden's index and for 50 and 100 ng/ml for daily smokers, or 25 and 50 ng/ml for occasional smokers.
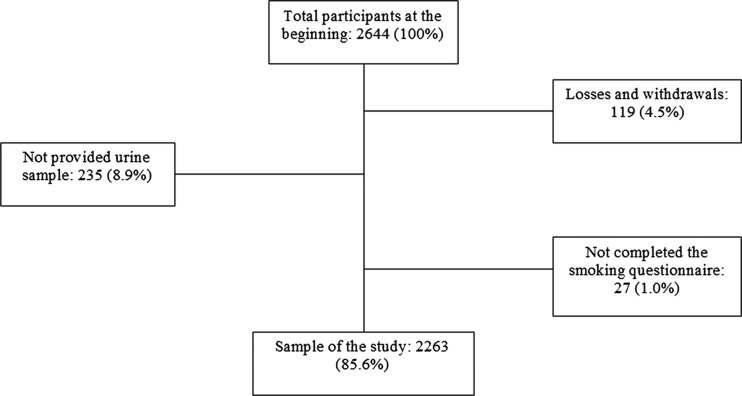
Participants: At the third trimester of pregnancy, 2263 pregnant women of the INMA Project were interviewed between 2004 and 2008 and a urine sample was collected.
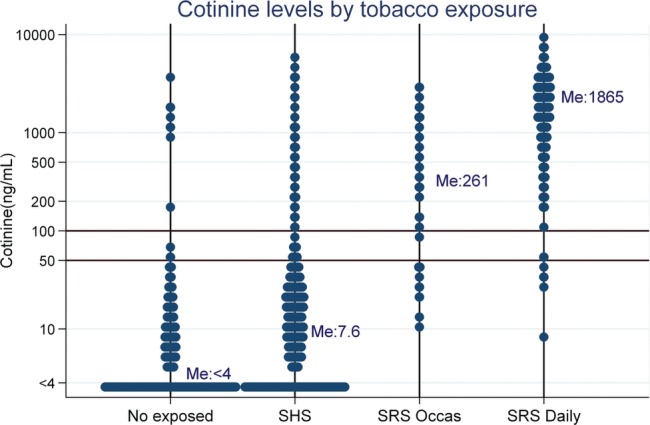
Results: Prevalence of self-reported smokers at the third trimester of pregnancy was 18.5%, and another 3.9% misreported their smoking status. Variables associated with self-reported smoking and misreporting were similar, including born in Europe, educational level and exposure to SHS. The optimal cut-off was 82 ng/ml (95% CI 42 to 133), sensitivity 95.2% and specificity 96.6%. The area under the ROC curve was 0.986 (95% CI 0.982 to 0.990). The cut-offs varied according to the SHS exposure level being 42 (95% CI 27 to 57), 82 (95% CI 46 to 136) and 106 ng/ml (95% CI 58 to 227) for not being SHS exposed, exposed to one, and to two or more sources of SHS, respectively. The optimal cut-off for discriminating occasional smokers from non-smokers was 27 ng/ml (95% CI 11 to 43).
Conclusions: Prevalence of smoking during pregnancy in Spain remains high. UC is a reliable biomarker for classifying pregnant women according to their smoking status. However, cut-offs would differ based on baseline exposure to SHS.
Figures
References
-
- Murin S, Rafii R, Bilello K. Smoking and smoking cessation in pregnancy. Clin Chest Med 2011;32:75–91 - PubMed
-
- Bardy AH, Seppälä T, Lillsunde P, et al. Objectively measured tobacco exposure during pregnancy: neonatal effects and relation to maternal smoking. Br J Obstet Gynaecol 1993;100:721–6 - PubMed
-
- Burstyn I, Kapur N, Shalapay C, et al. Evaluation of the accuracy of self-reported smoking in pregnancy when the biomarker level in an active smoker is uncertain. Nicotine Tob Res 2009;11:670–8 - PubMed
-
- Dietz PM, Homa D, England LJ, et al. Estimates of nondisclosure of cigarette smoking among pregnant and nonpregnant women of reproductive age in the United States. Am J Epidemiol 2011;173:355–9 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources