

Line bisection in Parkinson's disease: investigation of contributions of visual field, retinal vision, and scanning patterns to visuospatial function
- PMID: 23356329
- PMCID: PMC3762594
- DOI: 10.1037/a0031618
Line bisection in Parkinson's disease: investigation of contributions of visual field, retinal vision, and scanning patterns to visuospatial function
Abstract
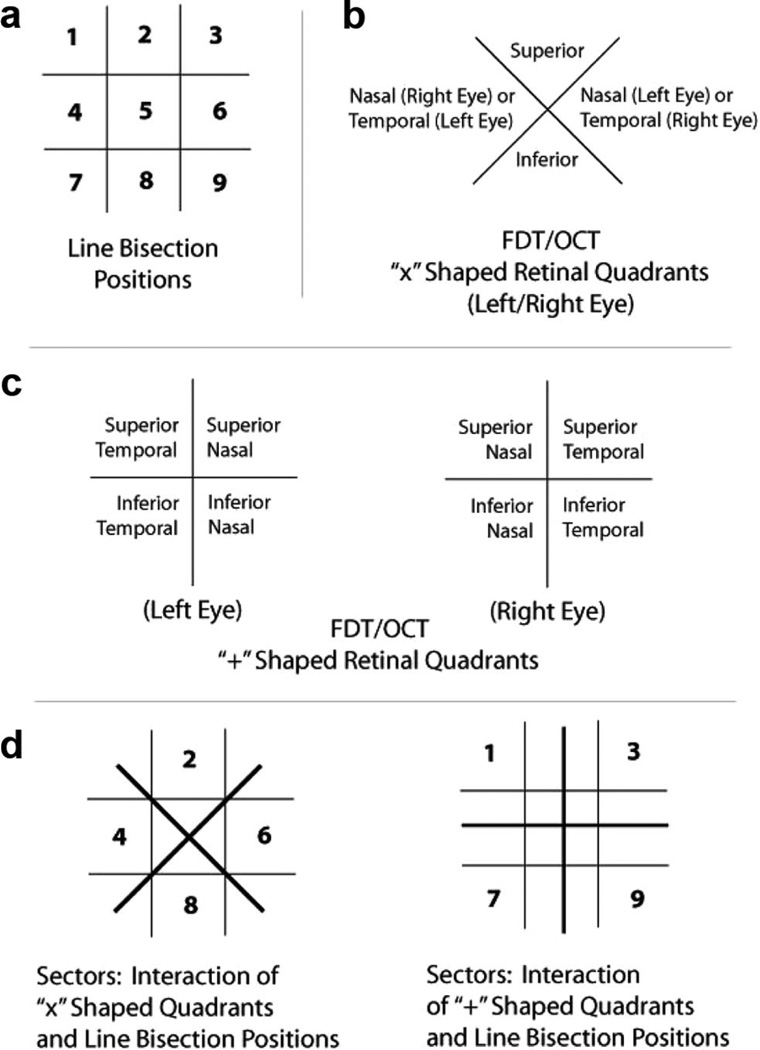
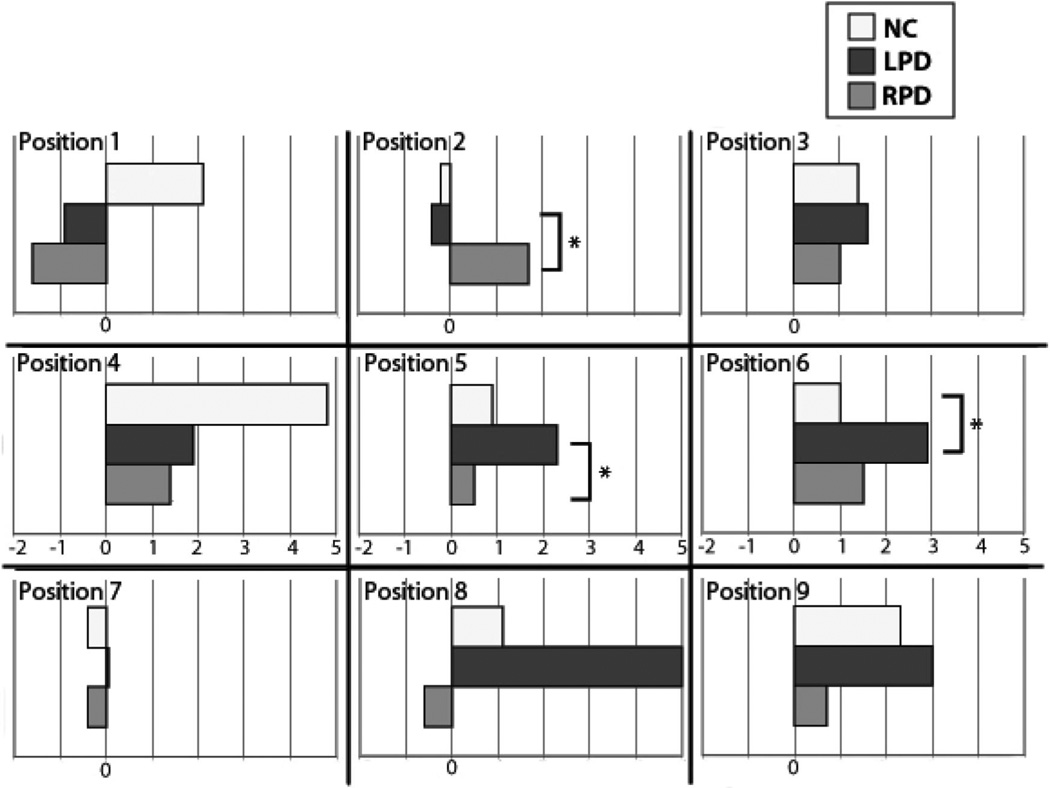
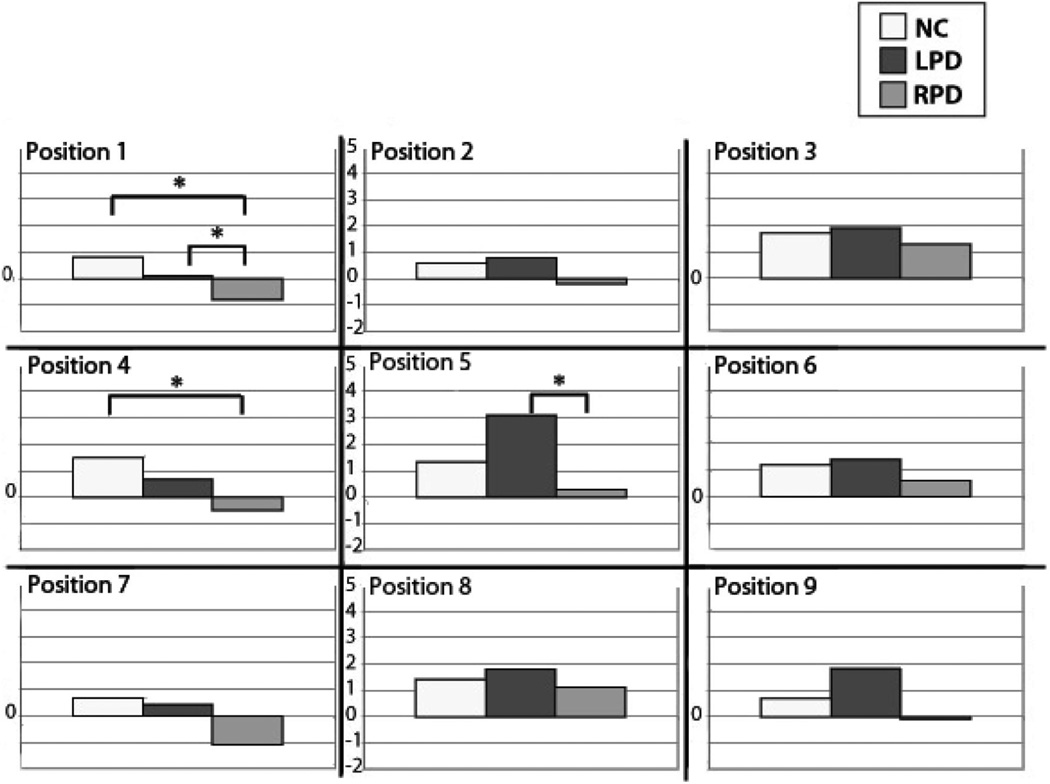
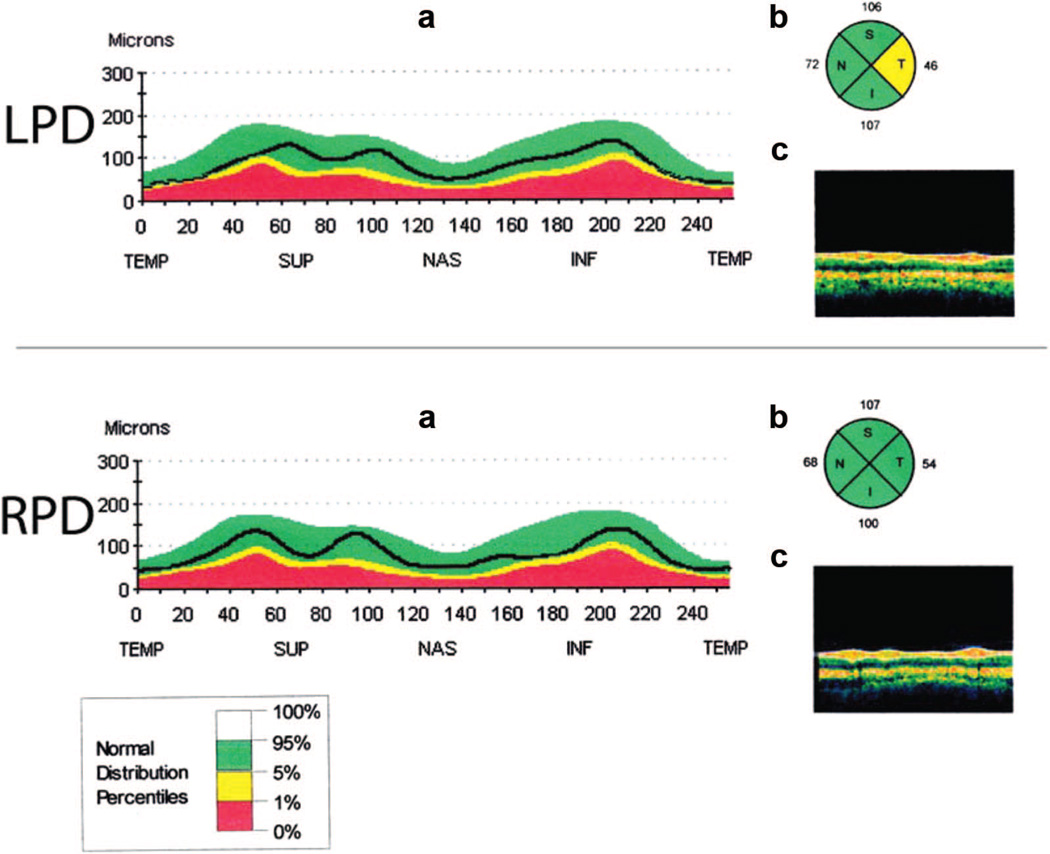
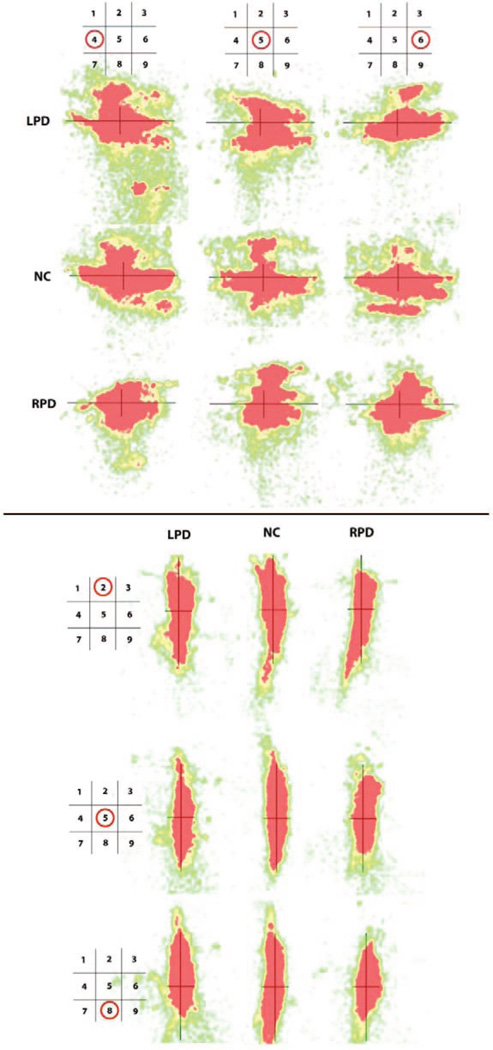
Parkinson's disease (PD) is characterized by disorders of visuospatial function that can impact everyday functioning. Visuospatial difficulties are more prominent in those whose motor symptoms begin on the left body side (LPD) than the right body side (RPD) and have mainly been attributed to parietal dysfunction. The source of visuospatial dysfunction is unclear, as in addition to subcortical-cortical changes, there are irregularities of visual scanning and potentially of retinal-level vision in PD. To assess these potential contributors, performance on a visuospatial task--line bisection--was examined together with retinal structure (nerve fiber layer thickness, measured by optical coherence tomography [OCT]), retinal function (contrast sensitivity, measured by frequency-doubling technology [FDT]), and visual scanning patterns. Participants included 20 nondemented patients (10 LPD, 10 RPD) and 11 normal control (NC) adults. Relative to the other groups, LPD were expected to show rightward bias on horizontal line bisection, especially within the left visual hemispace, and downward bias on vertical bisection. LPD relative rightward bias was confirmed, though not mainly within the left hemispace and not correlated with retinal structure or function. Retinal thinning was seen in LPD relative to RPD. Qualitative visualization of eye movements suggested greater LPD exploration of the right than left side of the line during horizontal bisection, and some overall compression of scanning range in RPD (both orientations) and LPD (primarily vertical). Results indicated that rightward visuospatial bias in our LPD sample arose not from abnormalities at the retinal level but potentially from attentional biases, reflected in eye movement patterns.
Figures
References
-
- Altintaş O, Işeri P, Ozkan B, Cağlar Y. Correlation between retinal morphological and functional findings and clinical severity in Parkinson’s disease. Documenta Opthalmologica. Advances in Ophthalmology. 2008;116:137–146. - PubMed
-
- Anderson AJ, Johnson CA. Frequency-doubling technology perimetry. Ophthalmology Clinics of North America. 2003;16:213–225. - PubMed
-
- Archibald NK, Clarke MP, Mosimann UP, Burn DJ. The retina in Parkinson’s disease. Brain: A Journal of Neurology. 2009;132:1128–1145. - PubMed
-
- Archibald NK, Clarke MP, Mosimann UP, Burn DJ. Retinal thickness in Parkinson’s disease. Parkinsonism & Related Disorders. 2011;17:431–436. - PubMed
-
- Barber J, Tomer R, Sroka H, Myslobodsky MS. Does unilateral dopamine deficit contribute to depression? Psychiatry Research. 1985;15:17–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
