

Effects of intravenous administration of allogenic bone marrow- and adipose tissue-derived mesenchymal stem cells on functional recovery and brain repair markers in experimental ischemic stroke
- PMID: 23356495
- PMCID: PMC3706777
- DOI: 10.1186/scrt159
Effects of intravenous administration of allogenic bone marrow- and adipose tissue-derived mesenchymal stem cells on functional recovery and brain repair markers in experimental ischemic stroke
Abstract
Introduction: Stem cell therapy can promote good recovery from stroke. Several studies have demonstrated that mesenchymal stem cells (MSC) are safe and effective. However, more information regarding appropriate cell type is needed from animal model. This study was targeted at analyzing the effects in ischemic stroke of acute intravenous (i.v.) administration of allogenic bone marrow- (BM-MSC) and adipose-derived-stem cells (AD-MSC) on functional evaluation results and brain repair markers.
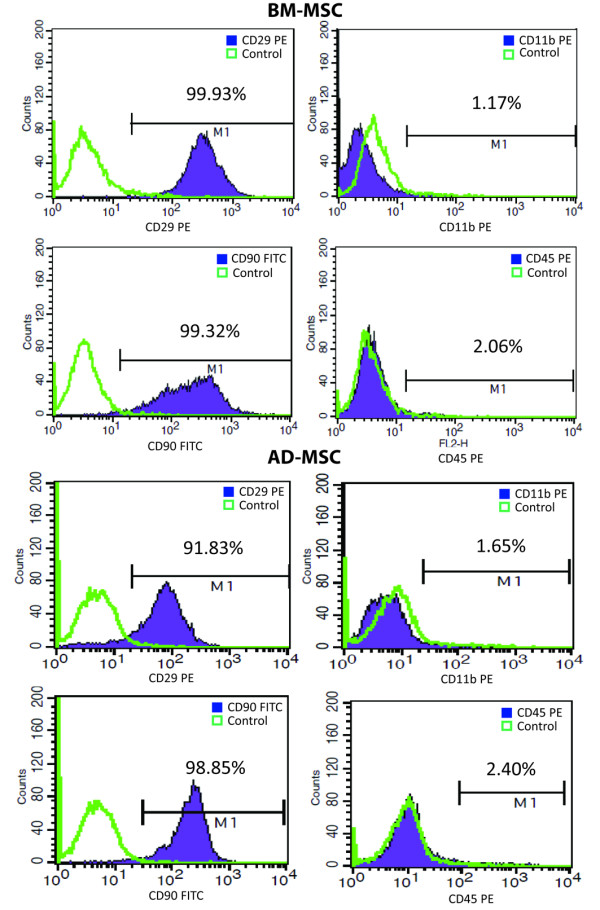
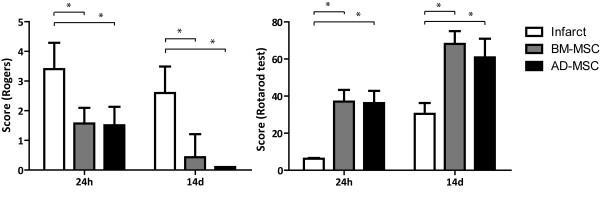
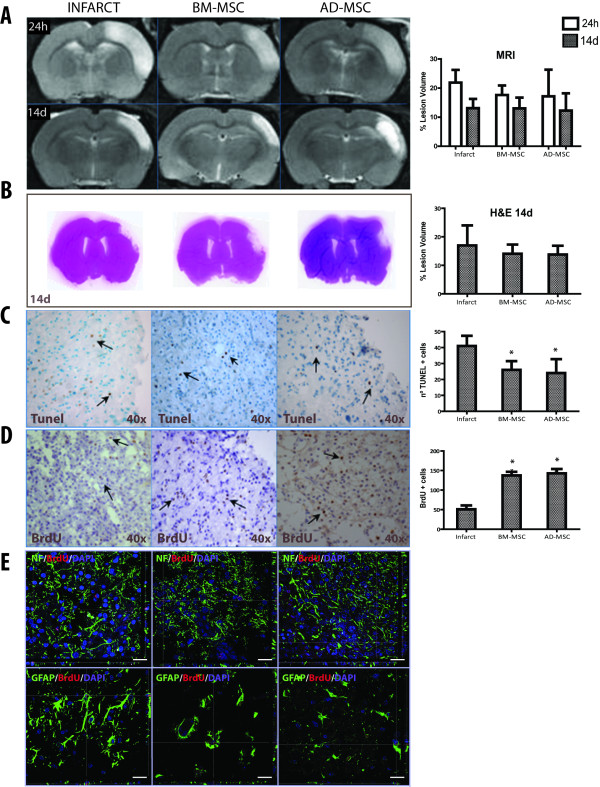
Methods: Allogenic MSC (2 × 106 cells) were administered intravenously 30 minutes after permanent middle cerebral artery occlusion (pMCAO) to rats. Infarct volume and cell migration and implantation were analyzed by magnetic resonance imaging (MRI) and immunohistochemistry. Function was evaluated by the Rogers and rotarod tests, and cell proliferation and cell-death were also determined. Brain repair markers were analyzed by confocal microscopy and confirmed by western blot.
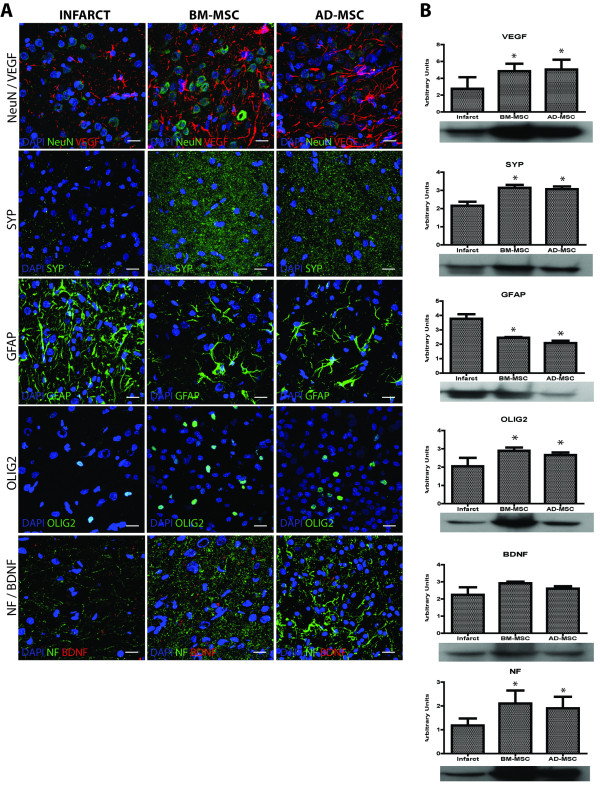
Results: Compared to infarct group, function had significantly improved at 24 h and continued at 14 d after i.v. administration of either BM-MSC or AD-MSC. No reduction in infarct volume or any migration/implantation of cells into the damaged brain were observed. Nevertheless, cell death was reduced and cellular proliferation significantly increased in both treatment groups with respect to the infarct group. At 14 d after MSC administration vascular endothelial growth factor (VEGF), synaptophysin (SYP), oligodendrocyte (Olig-2) and neurofilament (NF) levels were significantly increased while those of glial fiibrillary acid protein (GFAP) were decreased.
Conclusions: i.v. administration of allogenic MSC - whether BM-MSC or AD-MSC, in pMCAO infarct was associated with good functional recovery, and reductions in cell death as well as increases in cellular proliferation, neurogenesis, oligodendrogenesis, synaptogenesis and angiogenesis markers at 14 days post-infarct.
Figures
References
-
- Stem Cell Therapies as an Emerging Paradigm in Stroke Participants. Stem Cell Therapies as an Emerging Paradigm in Stroke (STEPS): bridging basic and clinical science for cellular and neurogenic factor therapy in treating stroke. Stroke. 2009;40:510–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
