

Randomized phase 2 trial to evaluate the clinical efficacy of two high-dosage tigecycline regimens versus imipenem-cilastatin for treatment of hospital-acquired pneumonia
- PMID: 23357775
- PMCID: PMC3623336
- DOI: 10.1128/AAC.01232-12
Randomized phase 2 trial to evaluate the clinical efficacy of two high-dosage tigecycline regimens versus imipenem-cilastatin for treatment of hospital-acquired pneumonia
Abstract
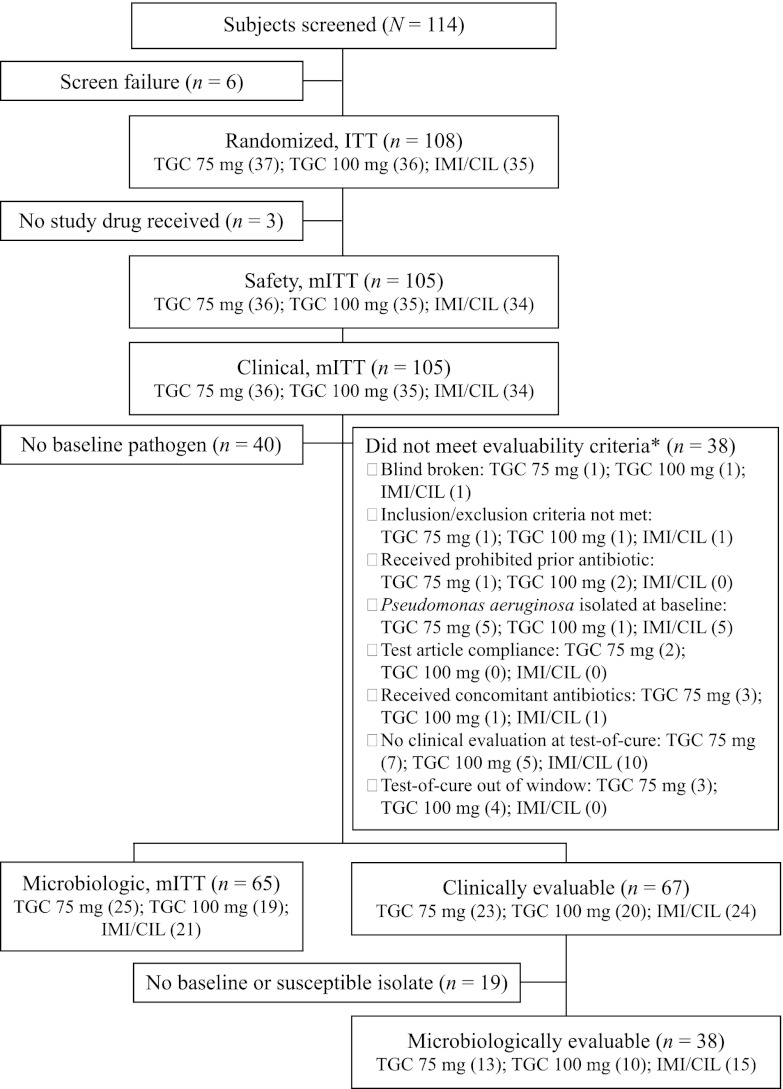
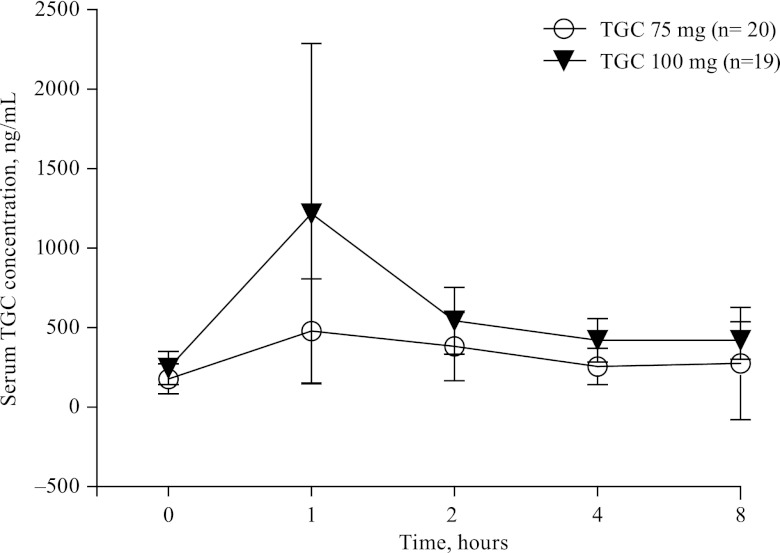
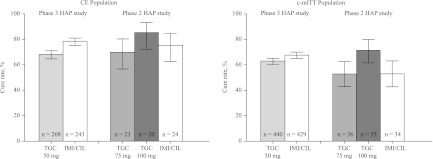
In a previous phase 3 study, the cure rates that occurred in patients with hospital-acquired pneumonia treated with tigecycline at the approved dose were lower than those seen with patients treated with imipenem and cilastatin (imipenem/cilastatin). We hypothesized that a higher dose of tigecycline is necessary in patients with hospital-acquired pneumonia. This phase 2 study compared the safety and efficacy of two higher doses of tigecycline with imipenem/cilastatin in subjects with hospital-acquired pneumonia. Subjects with hospital-acquired pneumonia were randomized to receive one of two doses of tigecycline (150 mg followed by 75 mg every 12 h or 200 mg followed by 100 mg every 12 h) or 1 g of imipenem/cilastatin every 8 h. Empirical adjunctive therapy was administered for initial coverage of methicillin-resistant Staphylococcus aureus and Pseudomonas aeruginosa infection, depending on the randomization regimen. Clinical response, defined as cure, failure of treatment, or indeterminate outcome, was assessed 10 to 21 days after the last day of therapy. In the clinically evaluable population, clinical cure with tigecycline 100 mg (17/20, 85.0%) was numerically higher than with tigecycline 75 mg (16/23, 69.6%) and imipenem/cilastatin (18/24, 75.0%). No new safety signals with the high-dose tigecycline were identified. A numerically higher clinical response was observed with the 100-mg dose of tigecycline. This supports our hypothesis that a higher area under the concentration-time curve over 24 h in the steady state divided by the MIC (AUC/MIC ratio) may be necessary to achieve clinical cure in patients with hospital-acquired pneumonia. Further studies are necessary. (The ClinicalTrials.gov identifier for this clinical trial is NCT00707239.).
Figures
References
-
- Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gibert C. 1996. Nosocomial pneumonia and mortality among patients in intensive care units. JAMA 275:866–869 - PubMed
-
- Ibrahim EH, Ward S, Sherman G, Kollef MH. 2000. A comparative analysis of patients with early-onset vs late-onset nosocomial pneumonia in the ICU setting. Chest 117:1434–1442 - PubMed
-
- Richards MJ, Edwards JR, Culver DH, Gaynes RP. 1999. Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System. Crit. Care Med. 27:887–892 - PubMed
-
- Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas-Chanoin MH, Wolff M, Spencer RC, Hemmer M. 1995. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. EPIC International Advisory Committee. JAMA 274:639–644 - PubMed
-
- Safdar N, Dezfulian C, Collard HR, Saint S. 2005. Clinical and economic consequences of ventilator-associated pneumonia: a systematic review. Crit. Care Med. 33:2184–2193 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
