

Sharing pain and relief: neural correlates of physicians during treatment of patients
- PMID: 23358155
- PMCID: PMC3981541
- DOI: 10.1038/mp.2012.195
Sharing pain and relief: neural correlates of physicians during treatment of patients
Abstract
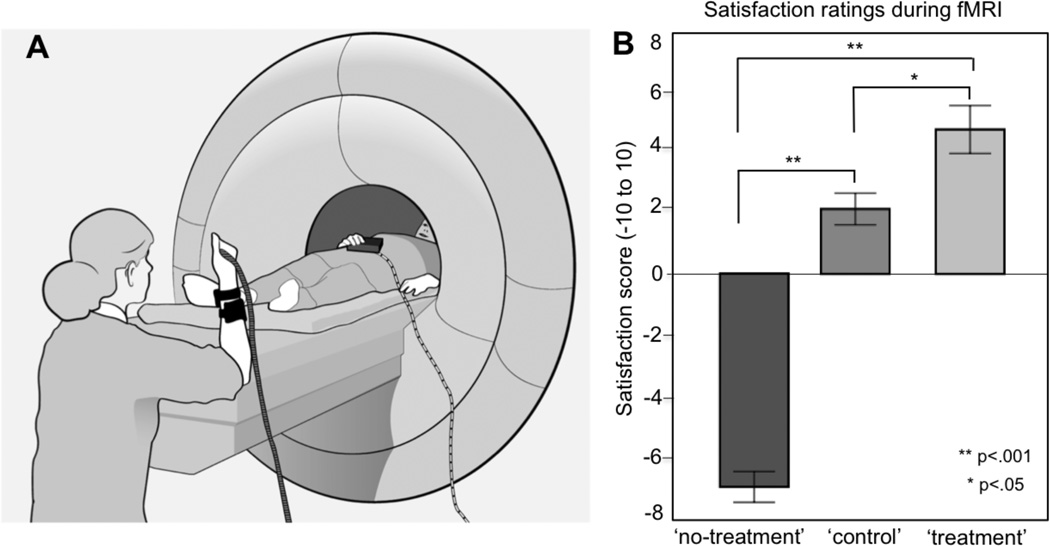
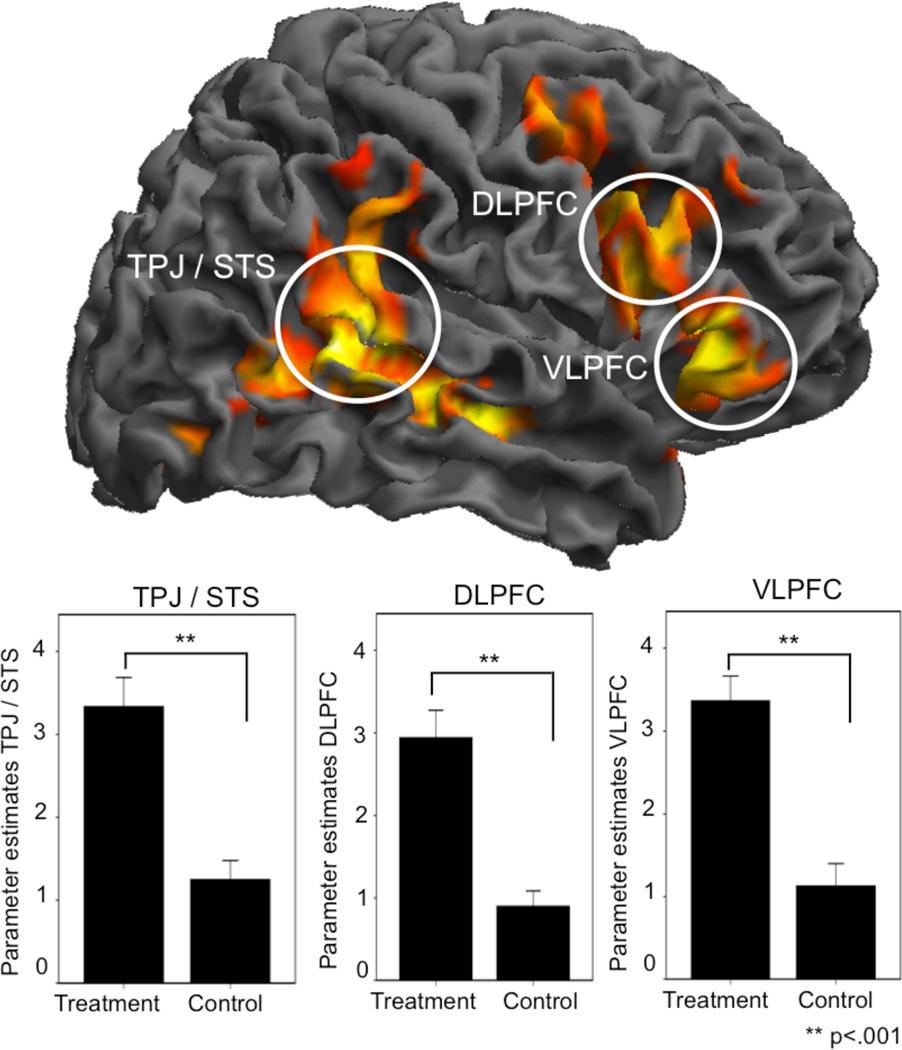
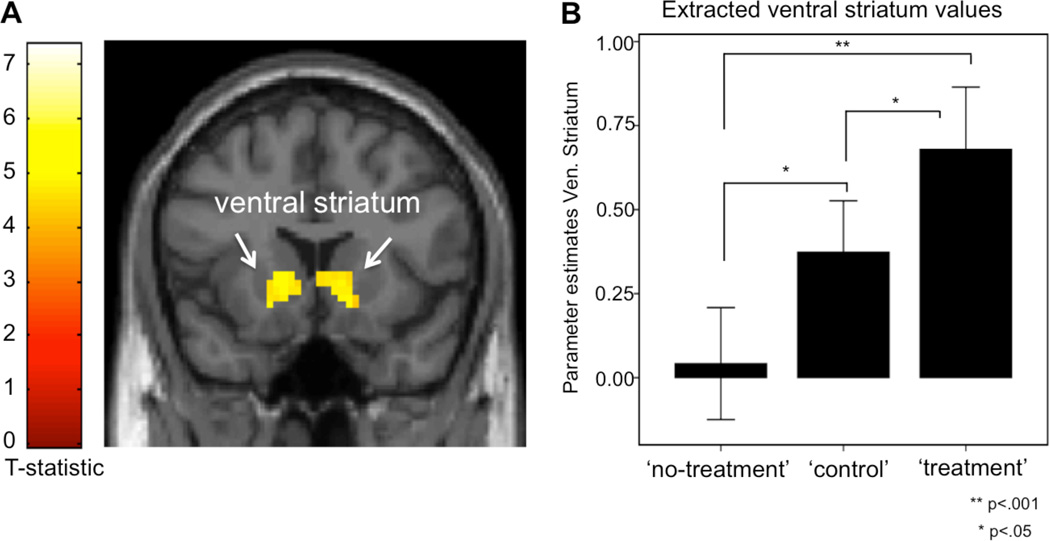
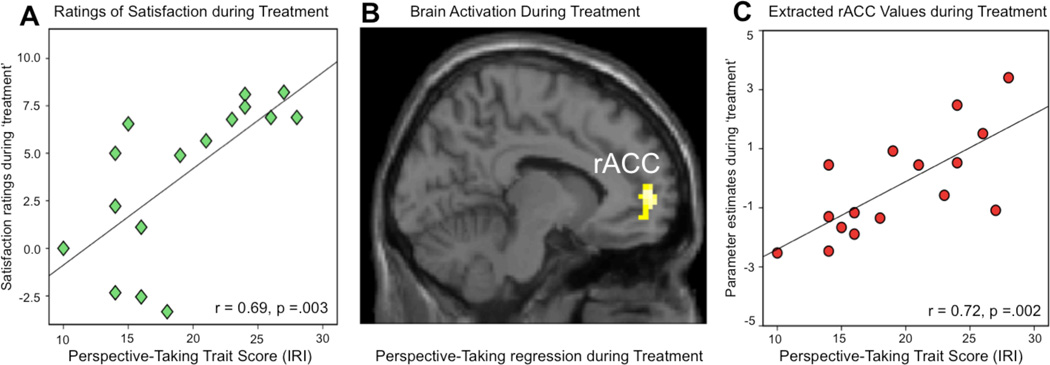
Patient-physician interactions significantly contribute to placebo effects and clinical outcomes. While the neural correlates of placebo responses have been studied in patients, the neurobiology of the clinician during treatment is unknown. This study investigated physicians' brain activations during patient-physician interaction while the patient was experiencing pain, including a 'treatment', 'no-treatment' and 'control' condition. Here, we demonstrate that physicians activated brain regions previously implicated in expectancy for pain-relief and increased attention during treatment of patients, including the right ventrolateral and dorsolateral prefrontal cortices. The physician's ability to take the patients' perspective correlated with increased brain activations in the rostral anterior cingulate cortex, a region that has been associated with processing of reward and subjective value. We suggest that physician treatment involves neural representations of treatment expectation, reward processing and empathy, paired with increased activation in attention-related structures. Our findings further the understanding of the neural representations associated with reciprocal interactions between clinicians and patients; a hallmark for successful treatment outcomes.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Finniss DG, Benedetti F. Mechanisms of the placebo response and their impact on clinical trials and clinical practice. Pain. 2005;114(1-2):3–6. - PubMed
-
- Pollo A, Amanzio M, Arslanian A, Casadio C, Maggi G, Benedetti F. Response expectancies in placebo analgesia and their clinical relevance. Pain. 2001;93(1):77–84. - PubMed
-
- Rief W, Nestoriuc Y, Weiss S, Welzel E, Barsky AJ, Hofmann SG. Metaanalysis of the placebo response in antidepressant trials. J Affect Disord. 2009;118(3):1–8. - PubMed
Publication types
MeSH terms
Grants and funding
- K01 AT003883/AT/NCCIH NIH HHS/United States
- P41 RR014075/RR/NCRR NIH HHS/United States
- K24 AT004095/AT/NCCIH NIH HHS/United States
- R21AT004497/AT/NCCIH NIH HHS/United States
- AT006663/AT/NCCIH NIH HHS/United States
- P01 AT006663/AT/NCCIH NIH HHS/United States
- R01AT005280/AT/NCCIH NIH HHS/United States
- R03AT218317/AT/NCCIH NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- P41RR14075/RR/NCRR NIH HHS/United States
- R01 AT005280/AT/NCCIH NIH HHS/United States
- R03 DA030512/DA/NIDA NIH HHS/United States
- R01 AT006364/AT/NCCIH NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- UL1 RR025758-01/RR/NCRR NIH HHS/United States
- R01 AT004662/AT/NCCIH NIH HHS/United States
- KO1AT003883/AT/NCCIH NIH HHS/United States
- R01AT006364/AT/NCCIH NIH HHS/United States
- M01-RR-01066/RR/NCRR NIH HHS/United States
- R21 AT004497/AT/NCCIH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
