

Contralesional motor deficits after unilateral stroke reflect hemisphere-specific control mechanisms
- PMID: 23358602
- PMCID: PMC3613707
- DOI: 10.1093/brain/aws283
Contralesional motor deficits after unilateral stroke reflect hemisphere-specific control mechanisms
Abstract
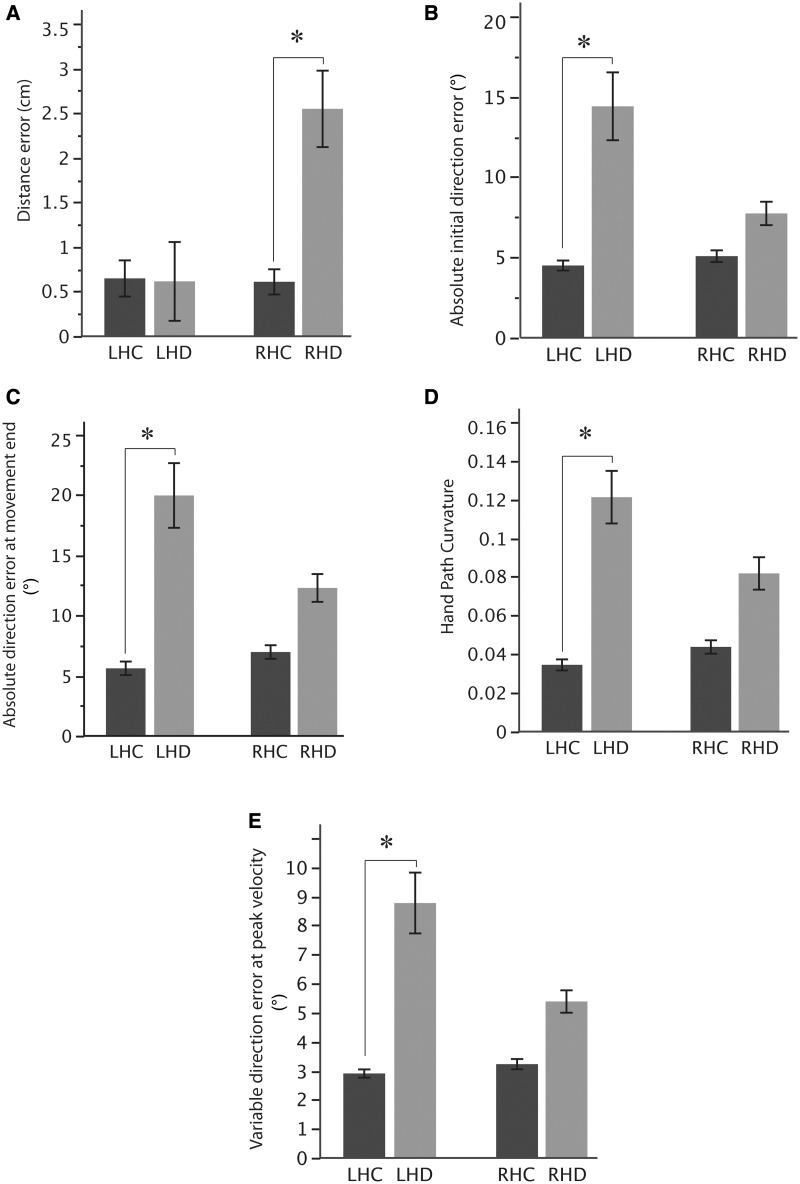
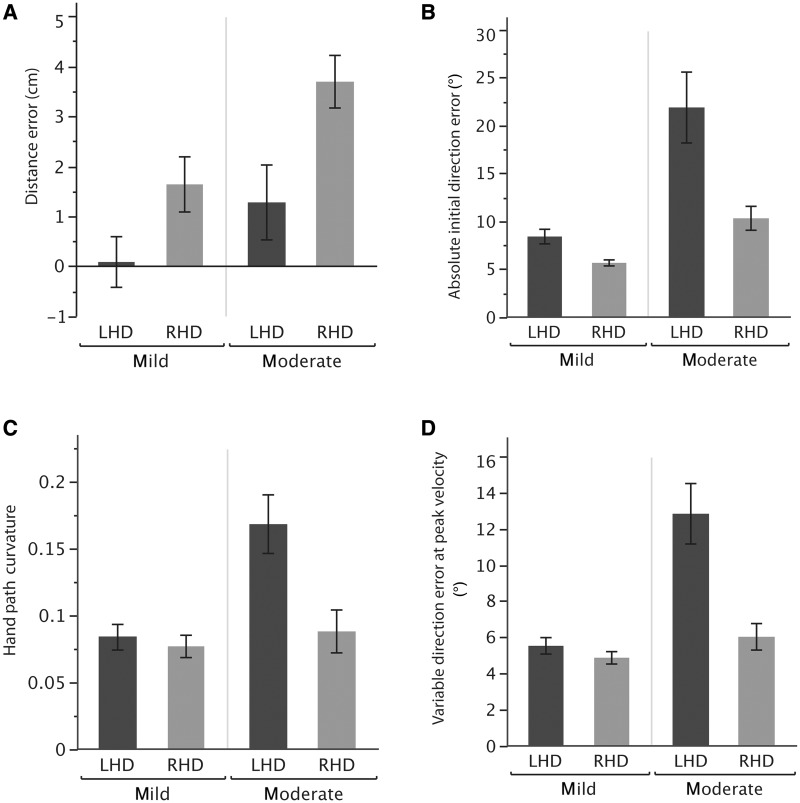
We have proposed a model of motor lateralization, in which the left and right hemispheres are specialized for different aspects of motor control: the left hemisphere for predicting and accounting for limb dynamics and the right hemisphere for stabilizing limb position through impedance control mechanisms. Our previous studies, demonstrating different motor deficits in the ipsilesional arm of stroke patients with left or right hemisphere damage, provided a critical test of our model. However, motor deficits after stroke are most prominent on the contralesional side. Post-stroke rehabilitation has also, naturally, focused on improving contralesional arm impairment and function. Understanding whether contralesional motor deficits differ depending on the hemisphere of damage is, therefore, of vital importance for assessing the impact of brain damage on function and also for designing rehabilitation interventions specific to laterality of damage. We, therefore, asked whether motor deficits in the contralesional arm of unilateral stroke patients reflect hemisphere-dependent control mechanisms. Because our model of lateralization predicts that contralesional deficits will differ depending on the hemisphere of damage, this study also served as an essential assessment of our model. Stroke patients with mild to moderate hemiparesis in either the left or right arm because of contralateral stroke and healthy control subjects performed targeted multi-joint reaching movements in different directions. As predicted, our results indicated a double dissociation; although left hemisphere damage was associated with greater errors in trajectory curvature and movement direction, errors in movement extent were greatest after right hemisphere damage. Thus, our results provide the first demonstration of hemisphere specific motor control deficits in the contralesional arm of stroke patients. Our results also suggest that it is critical to consider the differential deficits induced by right or left hemisphere lesions to enhance post-stroke rehabilitation interventions.
Figures
References
-
- Adamo DE, Alexander NB, Brown SH. The influence of age and physical activity on upper limb proprioceptive ability. J Aging Phys Act. 2009;17:272–93. - PubMed
-
- Albert ML. A simple test of visual neglect. Neurology. 1973;23:658–64. - PubMed
-
- Ashburner J, Friston KJ. Unified segmentation. NeuroImage. 2005;26:839–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
