

Managed problem solving for antiretroviral therapy adherence: a randomized trial
- PMID: 23358784
- PMCID: PMC5053821
- DOI: 10.1001/jamainternmed.2013.2152
Managed problem solving for antiretroviral therapy adherence: a randomized trial
Abstract
Background: Adherence to antiretroviral therapy is critical to successful treatment of human immunodeficiency virus (HIV). Few interventions have been demonstrated to improve both adherence and virologic outcomes. We sought to determine whether an intervention derived from problem solving theory, Managed Problem Solving (MAPS), would improve antiretroviral outcomes.
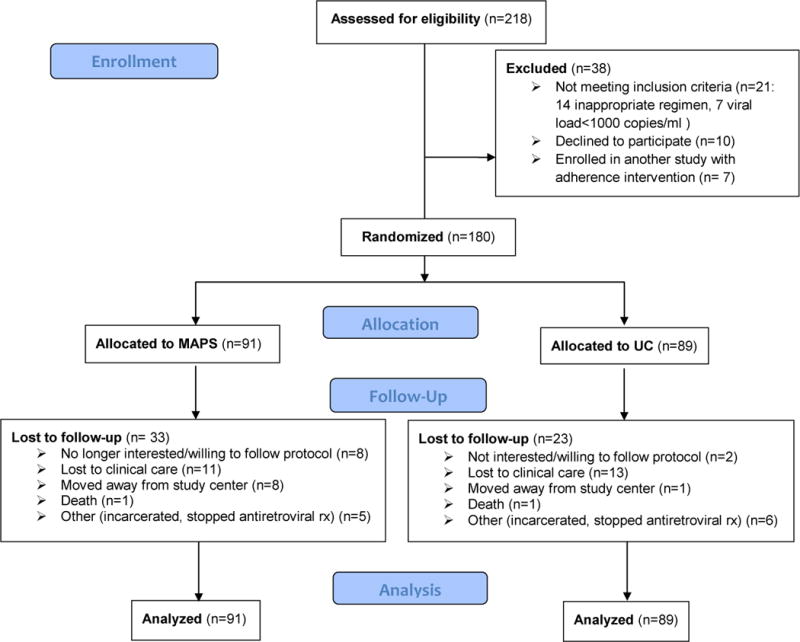
Methods: We conducted a randomized investigator blind trial of MAPS compared with usual care in HIV-1 infected individuals at 3 HIV clinics in Philadelphia, Pennsylvania. Eligible patients had plasma HIV-1 viral loads greater than 1000 copies/mL and were initiating or changing therapy. Managed Problem Solving consists of 4 in-person and 12 telephone-based meetings with a trained interventionist, then monthly follow-up calls for a year. Primary outcome was medication adherence measured using electronic monitors, summarized as fraction of doses taken quarterly over 1 year. Secondary outcome was undetectable HIV viral load over 1 year. We assessed 218 for eligibility, with 190 eligible and 180 enrolled, 91 randomized to MAPS and 89 to usual care. Fifty-six participants were lost to follow-up: 33 in the MAPS group and 23 in usual care group.
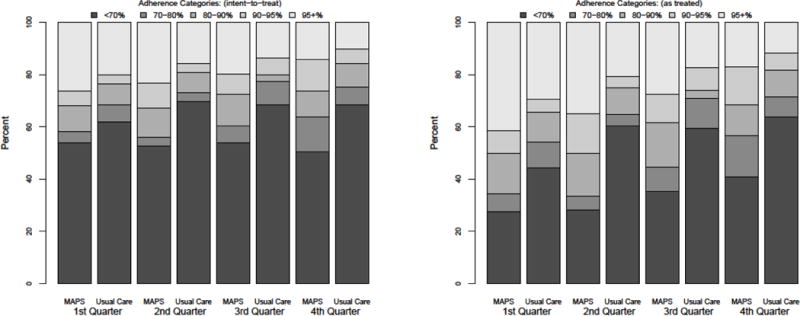
Results: In primary intention-to-treat analyses, the odds of being in a higher adherence category was 1.78 (95% CI,1.07-2.96) times greater for MAPS than usual care. In secondary analyses, the odds of an undetectable viral load was 1.48 (95% CI, 0.94-2.31) times greater for MAPS than usual care. In as-treated analyses, the effect of MAPS was stronger for both outcomes. There was neither a difference by prior treatment status nor change in effect over time.
Conclusions: Managed Problem Solving is an effective antiretroviral adherence intervention over the first year with a new regimen. It was equally effective at improving adherence in treatment experienced and naïve patients and did not lose effect over time. Implementation of MAPS should be strongly considered where resources are available.
Trial registration: clinicaltrials.gov Identifier: NCT00130273.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Lifetime HIV antiretroviral therapy adherence intervention: timing is everything: comment on "Managed problem solving for antiretroviral therapy adherence".JAMA Intern Med. 2013 Feb 25;173(4):306-7. doi: 10.1001/jamainternmed.2013.2858. JAMA Intern Med. 2013. PMID: 23358810 Free PMC article. No abstract available.
-
Does managed problem solving work and in what setting?JAMA Intern Med. 2013 Aug 12;173(15):1474. doi: 10.1001/jamainternmed.2013.7788. JAMA Intern Med. 2013. PMID: 23939522 No abstract available.
-
Reply: To PMID 23358784.JAMA Intern Med. 2013 Aug 12;173(15):1475-6. doi: 10.1001/jamainternmed.2013.7782. JAMA Intern Med. 2013. PMID: 23939524 Free PMC article. No abstract available.
References
-
- Asche C, LaFleur J, Conner C. A review of diabetes treatment adherence and the association with clinical and economic outcomes. Clin Ther. 2011;33:74–109. - PubMed
-
- Pittman DG, Tao Z, Chen W, Stettin GD. Antihypertensive medication adherence and subsequent healthcare utilization and costs. Am J Manag Care. 2010;16:568–576. - PubMed
-
- Chan DC, Shrank WH, Cutler D, Jan S, Fischer MA, et al. Patient, physician, and payment predictors of statin adherence. Med Care. 2010;48:196–202. - PubMed
-
- Gross R, Yip B, Re VL, 3rd, Wood E, Alexander CS, et al. A simple, dynamic measure of antiretroviral therapy adherence predicts failure to maintain HIV-1 suppression. J Infect Dis. 2006;194:1108–1114. - PubMed
-
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Archives of Internal Medicine. 2000;160:2101–2107. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
