

Surgical excision with left atrial reconstruction of a primary functioning retrocardiac paraganglioma
- PMID: 23360571
- PMCID: PMC3599281
- DOI: 10.1186/1749-8090-8-22
Surgical excision with left atrial reconstruction of a primary functioning retrocardiac paraganglioma
Abstract
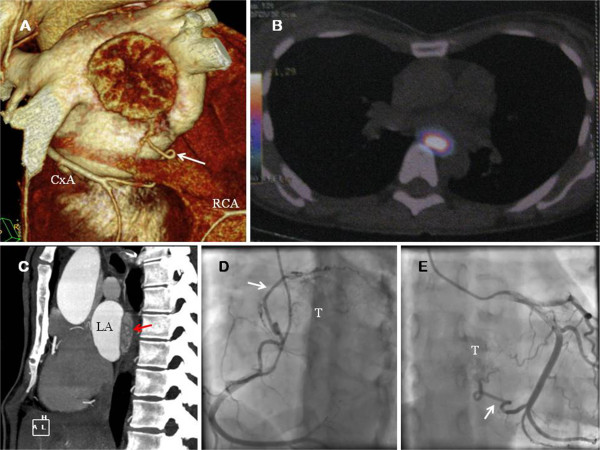
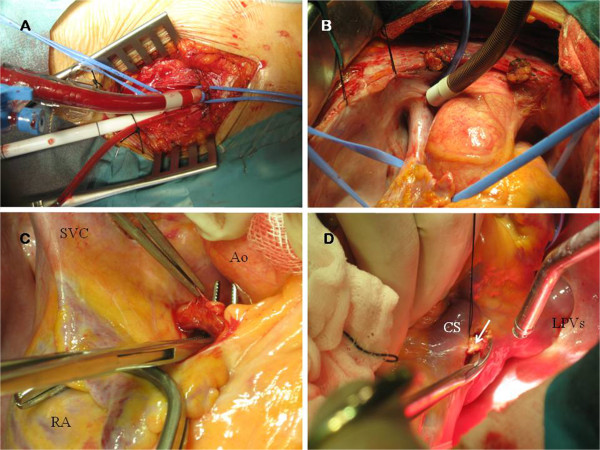
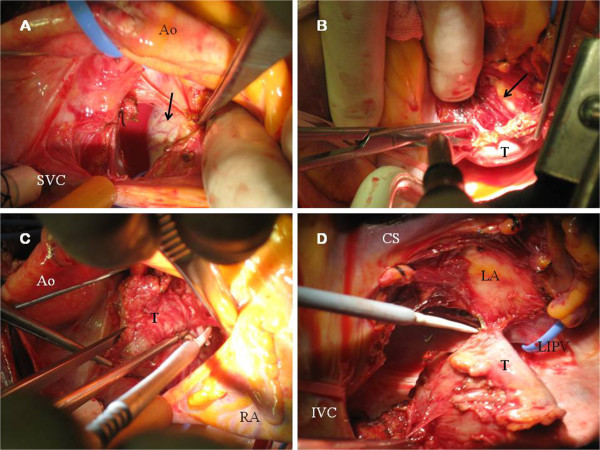
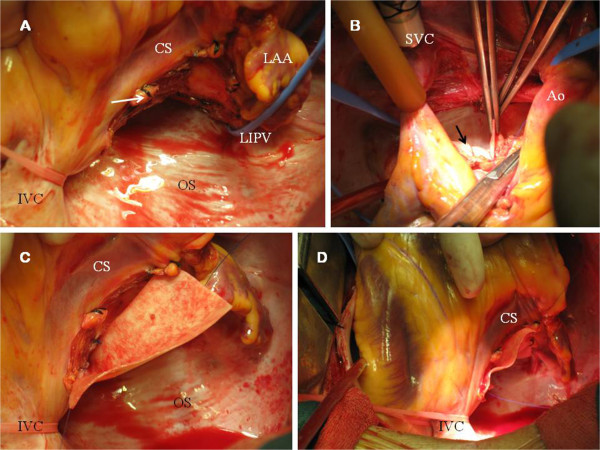
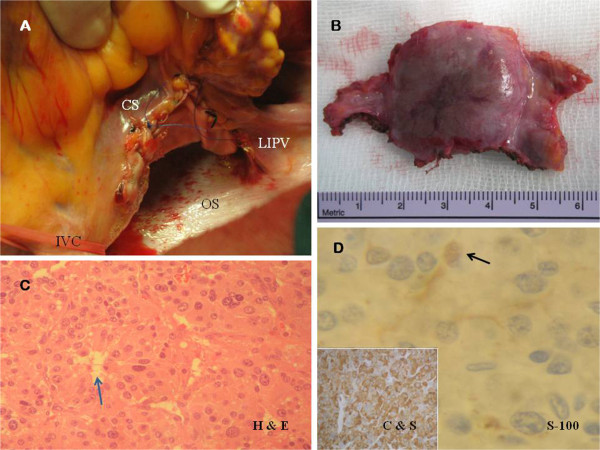
About 2% of all paragangliomas are located in the chest, and a few have been described to be found in the heart. Primary cardiac paragangliomas are extremely uncommon tumors and surgical experience with this neoplasm is limited. Treatment strategies described in the literature have included simple excision, excision with reconstruction, autotransplantation after excision of the tumor and even orthotopic cardiac transplantation, depending on the extent of disease. A primary retrocardiac paraganglioma catecholamine-productive was identified in an asymptomatic 49-year old female associated to familial pheochromocytoma-paraganglioma syndrome caused by germline mutation of the gen which codifies for the subunit B of succinate dehydrogenase enzyme (SDHB). The neoplasm was surgically excised from the posterior surface of the left atrium via median sternotomy using cardiopulmonary bypass. Direct ligation of feeding vessels of the tumor along with left atrial reinforcement using a pericardial patch was performed. The post-operative course was uneventful, with normalization of catecholamine secretion and no recurrence at three-month follow-up. We review the current literature about this exceptional cardiac tumor, pathophysiological conditions and options for surgical management.
Figures
References
-
- Pacheco N, Marcos G, Garcipérez FJ, Pérez C. Intrapericardial paraganglioma. Rev Esp Cardiol. 2010;63:116–117. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
