

Men's preferences for prostate cancer screening: a discrete choice experiment
- PMID: 23361056
- PMCID: PMC3593568
- DOI: 10.1038/bjc.2013.5
Men's preferences for prostate cancer screening: a discrete choice experiment
Abstract
Background: Screening for prostate cancer (PC) may save lives, but overdiagnosis and overtreatment are serious drawbacks. We aimed to determine men's preferences for PC screening, and to elicit the trade-offs they make.
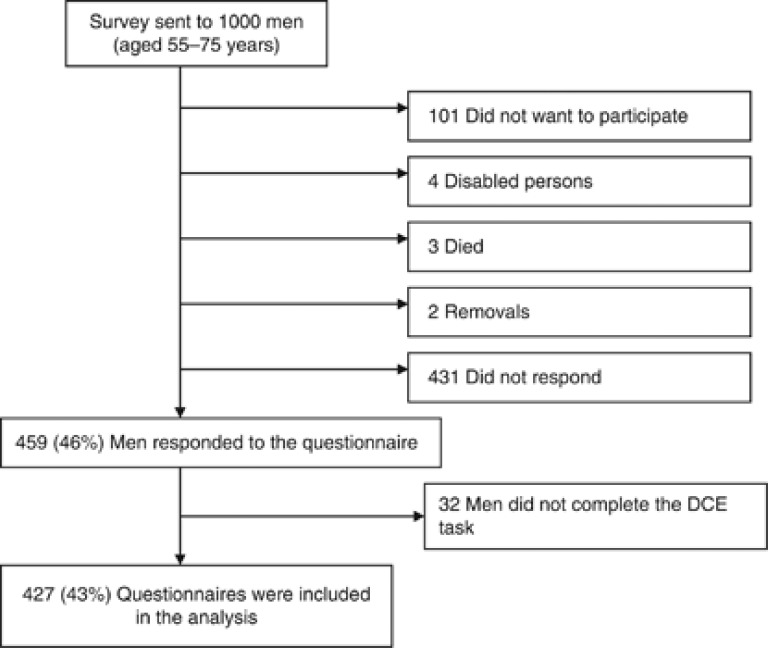
Methods: A discrete choice experiment (DCE) was conducted among a population-based random sample of 1000 elderly men (55-75-years-old). Trade-offs were quantified with a panel latent class model between five PC screening aspects: risk reduction of PC-related death, screening interval, risk of unnecessary biopsies, risk of unnecessary treatments, and out-of-pocket costs.
Results: The response rate was 46% (459/1000). Men were willing to trade-off 2.0% (CI: 1.6%-2.4%) or 1.8% (CI: 1.3%-2.3%) risk reduction of PC-related death to decrease their risk of unnecessary treatment or biopsy with 10%, respectively. They were willing to pay €188 per year (CI: €141-€258) to reduce their relative risk of PC-related death with 10%. Preference heterogeneity was substantial, with men with higher educational levels having a lower probability to opt for PC screening than men with lower educational levels.
Conclusion: Men were willing to trade-off some risk reduction of PC-related death to be relieved of the burden of biopsies or unnecessary treatments. Increasing knowledge on overdiagnosis and overtreatment, especially for men with lower educational levels, is warranted to prevent unrealistic expectations from PC screening.
Figures
References
-
- Andriole GL, Crawford ED, Grubb RL, Buys SS, Chia D, Church TR, Fouad MN, Gelmann EP, Kvale PA, Reding DJ, Weissfeld JL, Yokochi LA, O'Brien B, Clapp JD, Rathmell JM, Riley TL, Hayes RB, Kramer BS, Izmirlian G, Miller AB, Pinsky PF, Prorok PC, Gohagan JK, Berg CD. Mortality results from a randomized prostate-cancer screening trial. N Engl J Med. 2009;360:1310–1319. - PMC - PubMed
-
- Bech M, Kjaer T, Lauridsen J. Does the number of choice sets matter? Results from a web survey applying a discrete choice experiment. Health Econ. 2011;20:273–286. - PubMed
-
- Bishop AJ, Marteau TM, Armstrong D, Chitty LS, Longworth L, Buxton MJ, Berlin C. Women and health care professionals' preferences for Down's Syndrome screening tests: a conjoint analysis study. BJOG. 2004;111:775–779. - PubMed
-
- Daly A, Hess S, Train K. Assuring finite moments for willingness to pay in random coefficient models. Transportation. 2012;39:267–297.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
