

Tumor localization and biochemical response to cure in tumor-induced osteomalacia
- PMID: 23362135
- PMCID: PMC3900247
- DOI: 10.1002/jbmr.1881
Tumor localization and biochemical response to cure in tumor-induced osteomalacia
Abstract
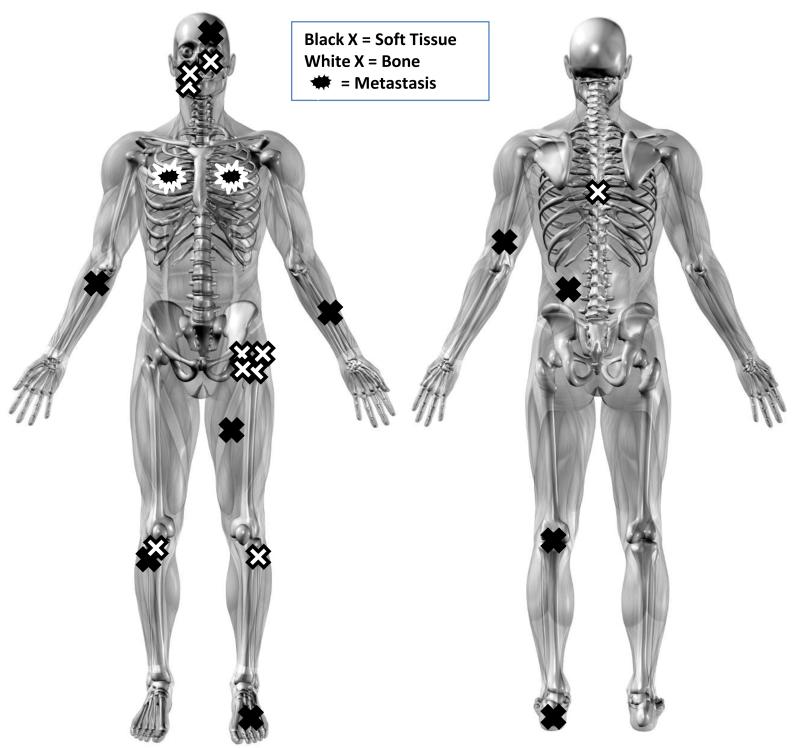
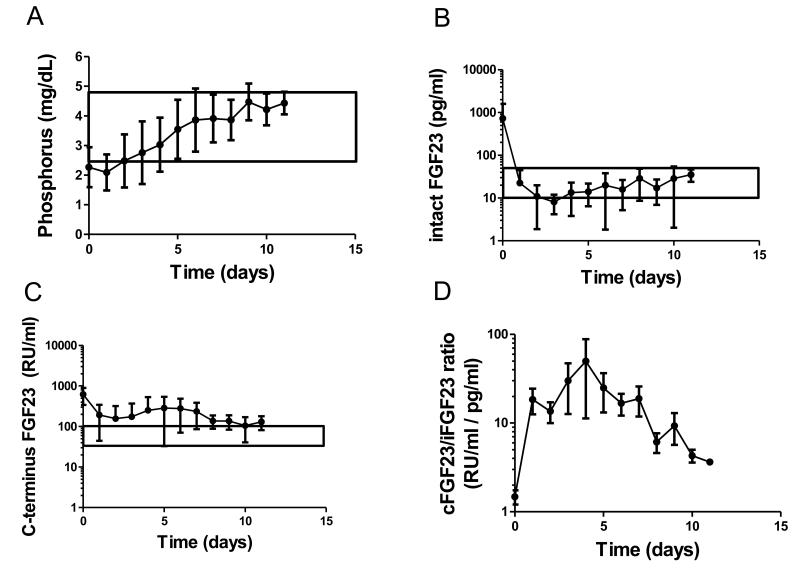
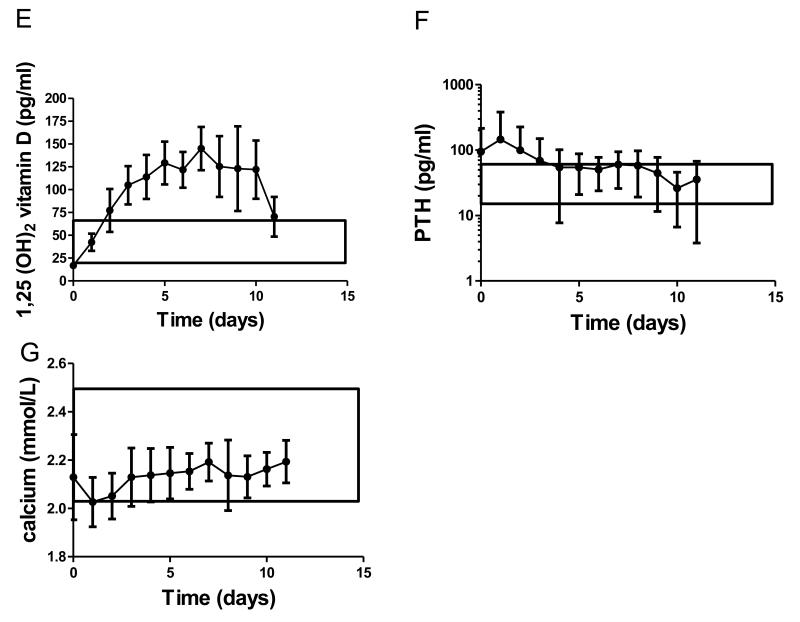
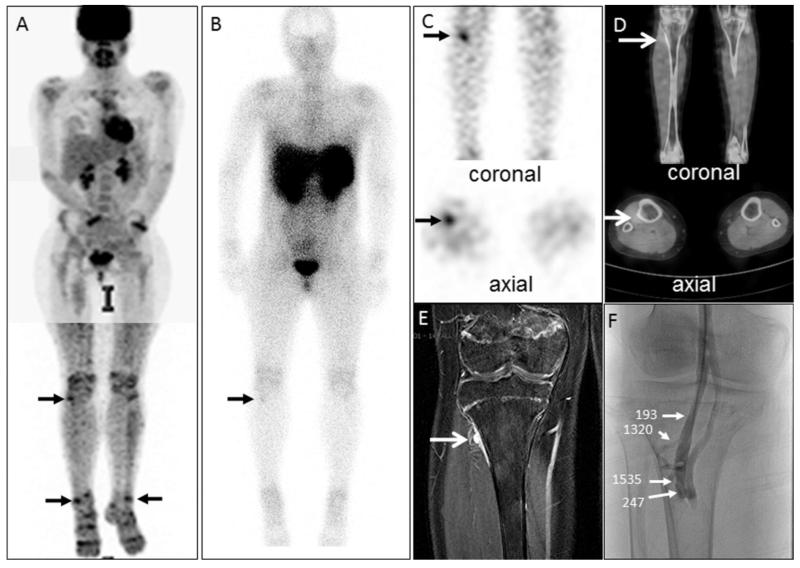
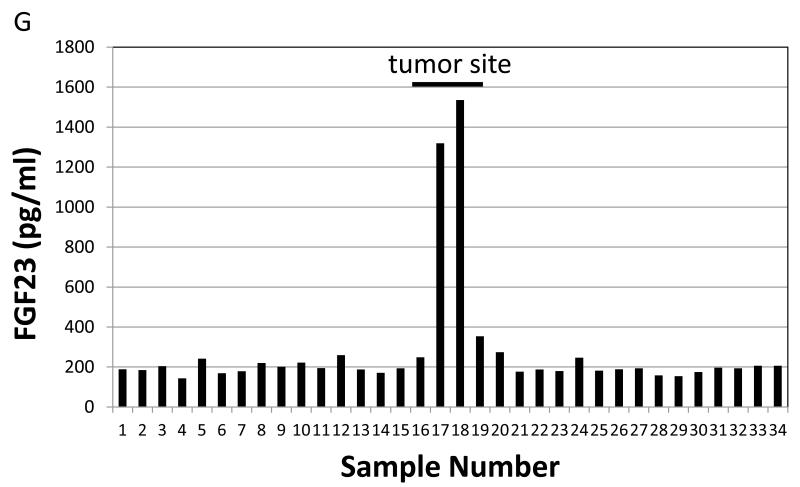
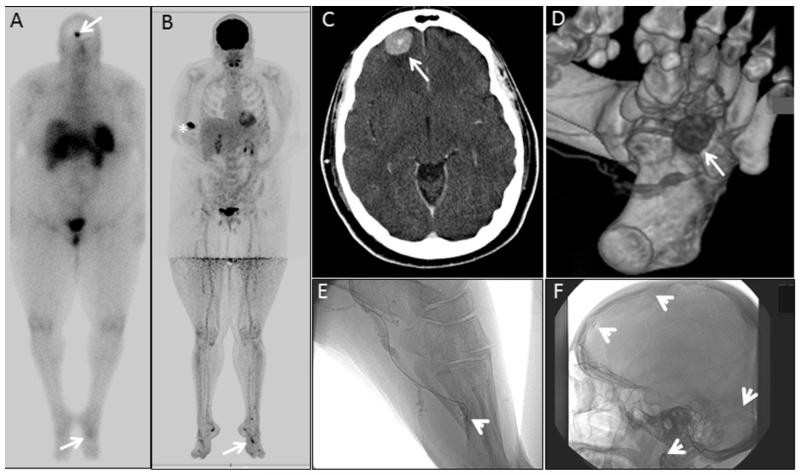
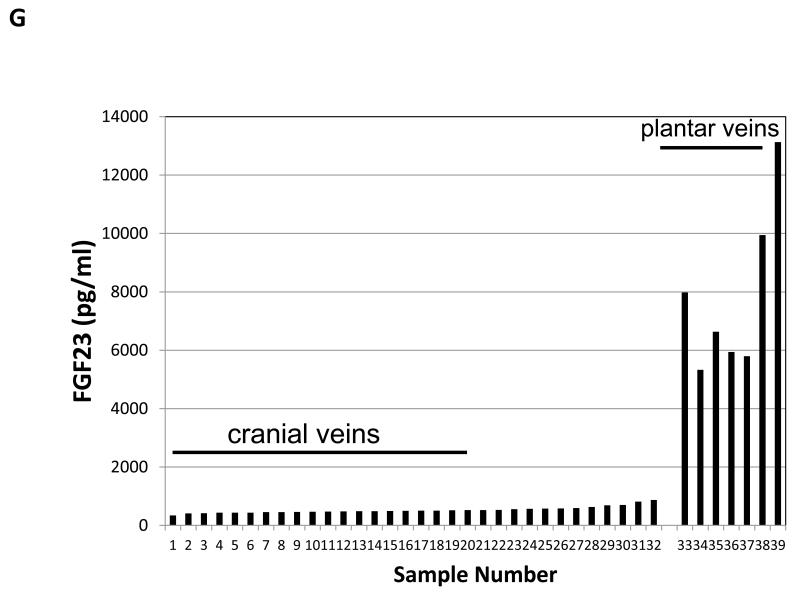
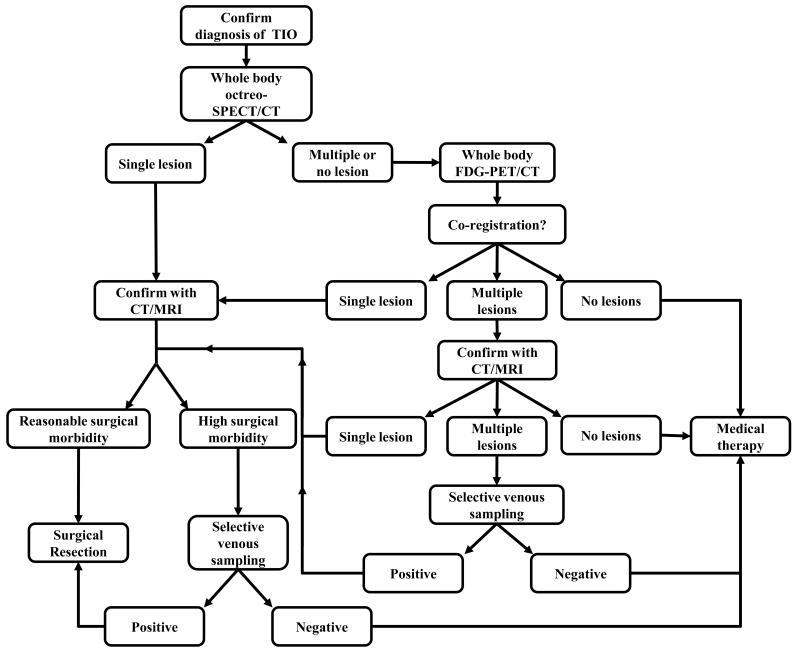
Tumor-induced osteomalacia (TIO) is a rare disorder of phosphate wasting due to fibroblast growth factor-23 (FGF23)-secreting tumors that are often difficult to locate. We present a systematic approach to tumor localization and postoperative biochemical changes in 31 subjects with TIO. All had failed either initial localization, or relocalization (in case of recurrence or metastases) at outside institutions. Functional imaging with ¹¹¹Indium-octreotide with single photon emission computed tomography (octreo-SPECT or SPECT/CT), and ¹⁸fluorodeoxyglucose positron emission tomography/CT (FDG-PET/CT) were performed, followed by anatomic imaging (CT, MRI). Selective venous sampling (VS) was performed when multiple suspicious lesions were identified or high surgical risk was a concern. Tumors were localized in 20 of 31 subjects (64.5%). Nineteen of 20 subjects underwent octreo-SPECT imaging, and 16 of 20 FDG-PET/CT imaging. Eighteen of 19 (95%) were positive on octreo-SPECT, and 14 of 16 (88%) on FDG-PET/CT. Twelve of 20 subjects underwent VS; 10 of 12 (83%) were positive. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were as follows: sensitivity = 0.95, specificity = 0.64, PPV = 0.82, and NPV = 0.88 for octreo-SPECT; sensitivity = 0.88, specificity = 0.36, PPV = 0.62, and NPV = 0.50 for FDG-PET/CT. Fifteen subjects had their tumor resected at our institution, and were disease-free at last follow-up. Serum phosphorus returned to normal in all subjects within 1 to 5 days. In 10 subjects who were followed for at least 7 days postoperatively, intact FGF23 (iFGF23) decreased to near undetectable within hours and returned to the normal range within 5 days. C-terminal FGF23 (cFGF23) decreased immediately but remained elevated, yielding a markedly elevated cFGF23/iFGF23 ratio. Serum 1,25-dihydroxyvitamin D₃ (1,25D) rose and exceeded the normal range. In this systematic approach to tumor localization in TIO, octreo-SPECT was more sensitive and specific, but in many cases FDG-PET/CT was complementary. VS can discriminate between multiple suspicious lesions and increase certainty prior to surgery. Sustained elevations in cFGF23 and 1,25D were observed, suggesting novel regulation of FGF23 processing and 1,25D generation.
Copyright © 2013 American Society for Bone and Mineral Research.
Figures
References
-
- Jan de Beur SM. Tumor-induced osteomalacia. Jama. 2005;294(10):1260–1267. - PubMed
-
- Drezner MK. Tumor-induced osteomalacia. Rev Endocr Metab Disord. 2001;2(2):175–186. - PubMed
-
- Folpe AL, Fanburg-Smith JC, Billings SD, Bisceglia M, Bertoni F, Cho JY, Econs MJ, Inwards CY, Jan de Beur SM, Mentzel T, Montgomery E, Michal M, Miettinen M, Mills SE, Reith JD, O’Connell JX, Rosenberg AE, Rubin BP, Sweet DE, Vinh TN, Wold LE, Wehrli BM, White KE, Zaino RJ, Weiss SW. Most osteomalacia-associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol. 2004;28(1):1–30. - PubMed
-
- Duet M, Kerkeni S, Sfar R, Bazille C, Liote F, Orcel P. Clinical impact of somatostatin receptor scintigraphy in the management of tumor-induced osteomalacia. Clin Nucl Med. 2008;33(11):752–756. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
