

Quantification of Mesenchymal Stem Cells (MSCs) at sites of human prostate cancer
- PMID: 23362217
- PMCID: PMC3702211
- DOI: 10.18632/oncotarget.805
Quantification of Mesenchymal Stem Cells (MSCs) at sites of human prostate cancer
Abstract
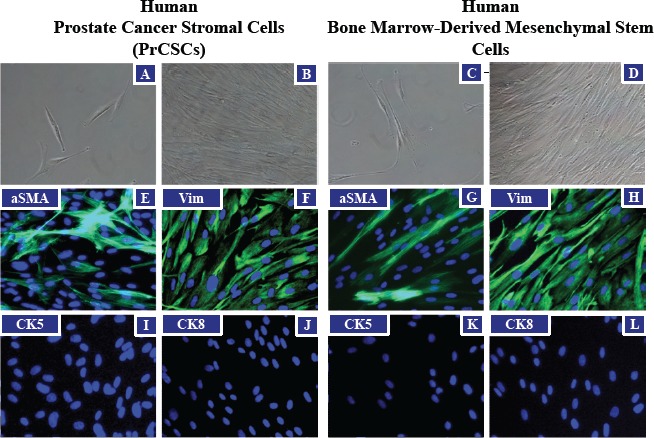
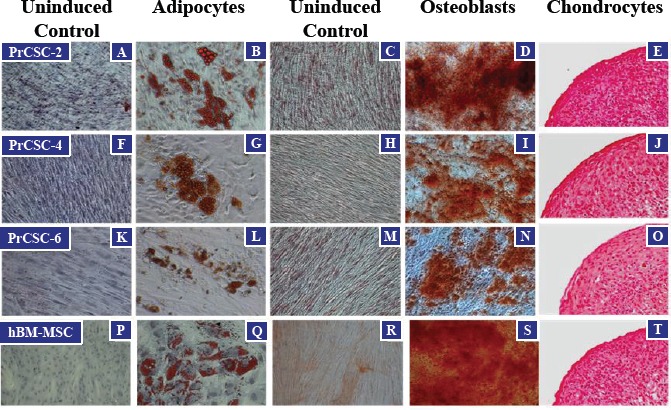
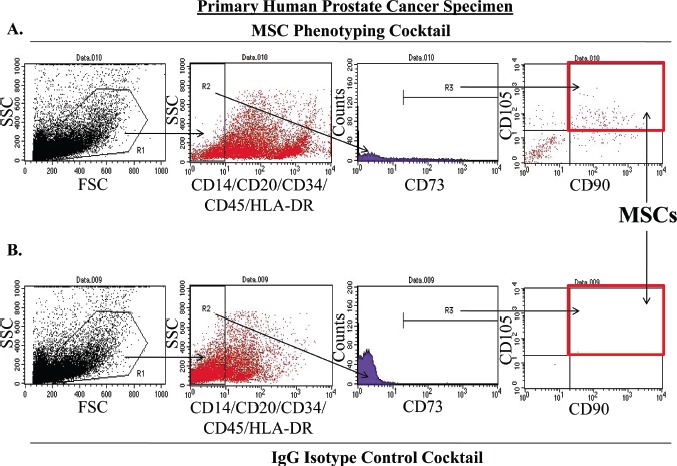
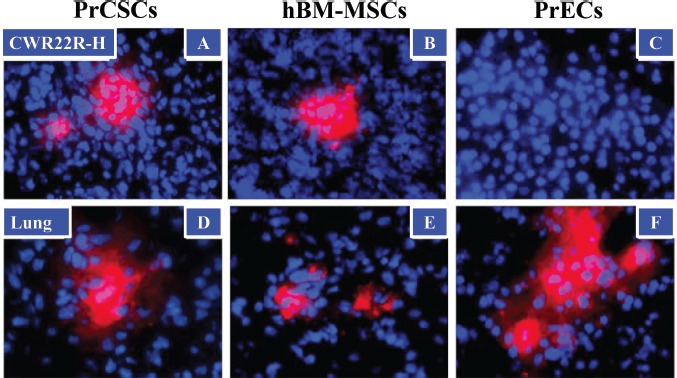
Circulating bone marrow-derived Mesenchymal Stem Cells (BM-MSCs) have an innate tropism for tumor tissue in response to the inflammatory microenvironment present in malignant lesions. The prostate is bombarded by numerous infectious and inflammatory insults over a lifetime. Chronic inflammation is associated with CXCL12, CCL5, and CCL2, which are highly overexpressed in prostate cancer. Among other cell types, these chemoattractant stimuli recruit BM-MSCs to the tumor. MSCs are minimally defined as plastic-adhering cells characterized by the expression of CD90, CD73, and CD105 in the absence of hematopoietic markers, which can differentiate into osteoblasts, chondrocytes, and adipocytes. MSCs are immunoprivileged and have been implicated in tumorigenesis through multiple mechanisms, including promoting proliferation, angiogenesis, and metastasis, in addition to the generation of an immunosuppressive microenvironment. We have demonstrated that MSCs represent 0.01-1.1% of the total cells present in core biopsies from primary human prostatectomies. Importantly, these analyses were performed on samples prior to expansion in tissue culture. MSCs in these prostatectomy samples are FAP-, CD90-, CD73-, and CD105-positive, and CD14-, CD20-, CD34-, CD45-, and HLA-DR-negative. Additionally, like BM-MSCs, these prostate cancer-derived stromal cells (PrCSCs) were shown to differentiate into osteoblasts, adipocytes and chondrocytes. In contrast to primary prostate cancer-derived epithelial cells, fluorescently-labeled PrCSCs and BM-MSCs were both shown to home to CWR22RH prostate cancer xenografts following IV injection. These studies demonstrate that not only are MSCs present in sites of prostate cancer where they may contribute to carcinogenesis, but these cells may also potentially be used to deliver cytotoxic or imaging agents for therapeutic and/or diagnostic purposes.
Figures
References
-
- English K, Mahon BP. Allogeneic mesenchymal stem cells: agents of immune modulation. J Cell Biochem. 2011;112(8):1963–1968. - PubMed
-
- Bianchi G, Borgonovo G, Pistoia V, Raffaghello L. Immunosuppressive cells and tumour microenvironment: focus on mesenchymal stem cells and myeloid derived suppressor cells. Histol Histopathol. 2011;26(7):941–951. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
