

Add-on effect of chinese herbal medicine on mortality in myocardial infarction: systematic review and meta-analysis of randomized controlled trials
- PMID: 23365612
- PMCID: PMC3556418
- DOI: 10.1155/2013/675906
Add-on effect of chinese herbal medicine on mortality in myocardial infarction: systematic review and meta-analysis of randomized controlled trials
Abstract
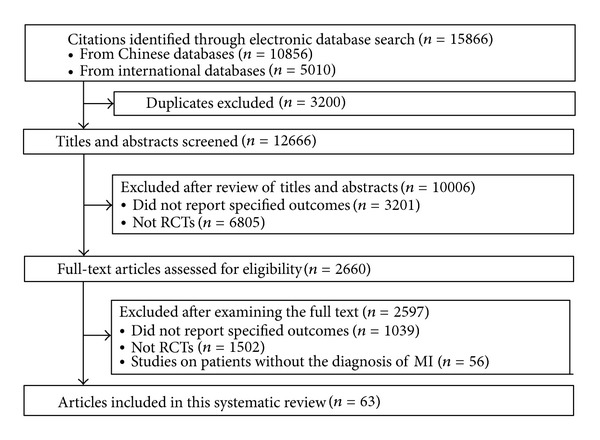
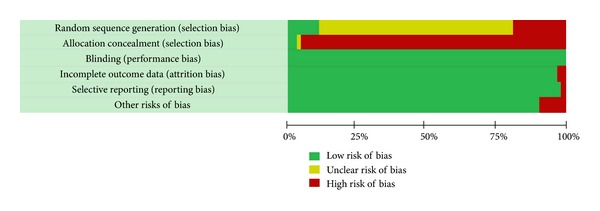
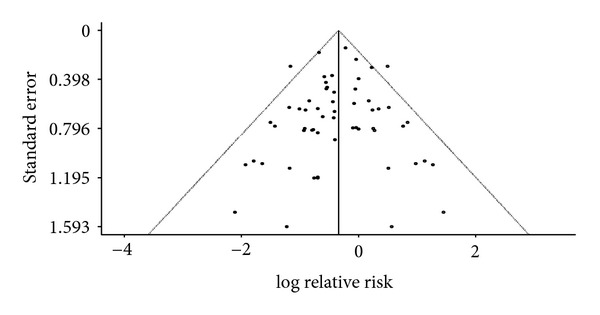
In China, Chinese herbal medicine (CHM) is widely used as an adjunct to biomedicine (BM) in treating myocardial infarction (MI). This meta-analysis of RCTs evaluated the efficacy of combined CHM-BM in the treatment of MI, compared to BM alone. Sixty-five RCTs (12,022 patients) of moderate quality were identified. 6,036 patients were given CHM plus BM, and 5,986 patients used BM only. Combined results showed clear additional effect of CHM-BM treatment in reducing all-cause mortality (relative risk reduction (RRR) = 37%, 95% CI = 28%-45%, I(2) = 0.0%) and mortality of cardiac origin (RRR = 39%, 95% CI = 22%-52%, I(2) = 22.8). Benefits remained after random-effect trim and fill adjustment for publication bias (adjusted RRR for all-cause mortality = 29%, 95% CI = 16%-40%; adjusted RRR for cardiac death = 32%, 95% CI = 15%-46%). CHM is also found to be efficacious in lowering the risk of fatal and nonfatal cardiogenic shock, cardiac arrhythmia, myocardial reinfarction, heart failure, angina, and occurrence of total heart events. In conclusion, addition of CHM is very likely to be able to improve survival of MI patients who are already receiving BM. Further confirmatory evaluation via large blinded randomized trials is warranted.
Figures
Similar articles
-
Evaluation of the add-on effect of chinese patent medicine for patients with stable or unstable angina: a systematic review and meta-analysis.Evid Based Complement Alternat Med. 2013;2013:673193. doi: 10.1155/2013/673193. Epub 2013 Dec 12. Evid Based Complement Alternat Med. 2013. PMID: 24416066 Free PMC article. Review.
-
The effect of Chinese herbal medicine on hemorrhagic shock: A systematic review and meta-analysis.Complement Ther Med. 2016 Dec;29:78-88. doi: 10.1016/j.ctim.2016.09.014. Epub 2016 Sep 12. Complement Ther Med. 2016. PMID: 27912961
-
Chinese Herbal Medicine Combined With First-Generation EGFR-TKIs in Treatment of Advanced Non-Small Cell Lung Cancer With EGFR Sensitizing Mutation: A Systematic Review and Meta-Analysis.Front Pharmacol. 2021 Aug 27;12:698371. doi: 10.3389/fphar.2021.698371. eCollection 2021. Front Pharmacol. 2021. PMID: 34512332 Free PMC article. Review.
-
Chinese herbal medicine for epidermal growth factor receptor inhibitor-induced skin rash in patients with malignancy: An updated meta-analysis of 23 randomized controlled trials.Complement Ther Med. 2019 Dec;47:102167. doi: 10.1016/j.ctim.2019.08.001. Epub 2019 Sep 9. Complement Ther Med. 2019. PMID: 31780021
-
Efficacy and Safety of Chinese Herbal Medicine on Ovarian Cancer After Reduction Surgery and Adjuvant Chemotherapy: A Systematic Review and Meta-Analysis.Front Oncol. 2019 Aug 16;9:730. doi: 10.3389/fonc.2019.00730. eCollection 2019. Front Oncol. 2019. PMID: 31475101 Free PMC article.
Cited by
-
Traditional Chinese Medicine for Acute Myocardial Infarction in Western Medicine Hospitals in China.Circ Cardiovasc Qual Outcomes. 2018 Mar;11(3):e004190. doi: 10.1161/CIRCOUTCOMES.117.004190. Circ Cardiovasc Qual Outcomes. 2018. PMID: 29848478 Free PMC article.
-
Shexiang Baoxin pills promotes angiogenesis in myocardial infarction rats via up-regulation of 20-HETE-mediated endothelial progenitor cells mobilization.Atherosclerosis. 2017 Aug;263:184-191. doi: 10.1016/j.atherosclerosis.2017.06.012. Epub 2017 Jun 7. Atherosclerosis. 2017. PMID: 28646793 Free PMC article.
-
Uncertain Associations of Major Bleeding and Concurrent Use of Antiplatelet Agents and Chinese Medications: A Nested Case-Crossover Study.Evid Based Complement Alternat Med. 2017;2017:9417186. doi: 10.1155/2017/9417186. Epub 2017 Aug 2. Evid Based Complement Alternat Med. 2017. PMID: 28831288 Free PMC article.
-
Expecting the holistic regulation from Chinese medicine based on the "solar system" hypothesis of ischemic heart disease.Chin J Integr Med. 2016 Nov;22(11):805-810. doi: 10.1007/s11655-016-2267-x. Epub 2016 Oct 26. Chin J Integr Med. 2016. PMID: 27783319 Review.
-
Traditional Chinese Medicine for Coronary Heart Disease: Clinical Evidence and Possible Mechanisms.Front Pharmacol. 2019 Aug 2;10:844. doi: 10.3389/fphar.2019.00844. eCollection 2019. Front Pharmacol. 2019. PMID: 31427964 Free PMC article.
References
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. - PubMed
-
- Unverzagt S, Hirsch K, Buerke M, et al. Inotropic agents and vasodilator strategies for acute myocardial infarction complicated by cardiogenic shock or low cardiac output syndrome (Protocol) Cochrane Database of Systematic Reviews. 2012;(2)CD009669 - PubMed
-
- Tang JL, Liu BY, Ma KW. Traditional Chinese medicine. The Lancet. 2008;372(9654):1938–1940. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
