

Unusual appearance and presentation of supratentorial subependymoma in an adult patient
- PMID: 23365712
- PMCID: PMC3558270
- DOI: 10.3941/jrcr.v6i8.999
Unusual appearance and presentation of supratentorial subependymoma in an adult patient
Abstract
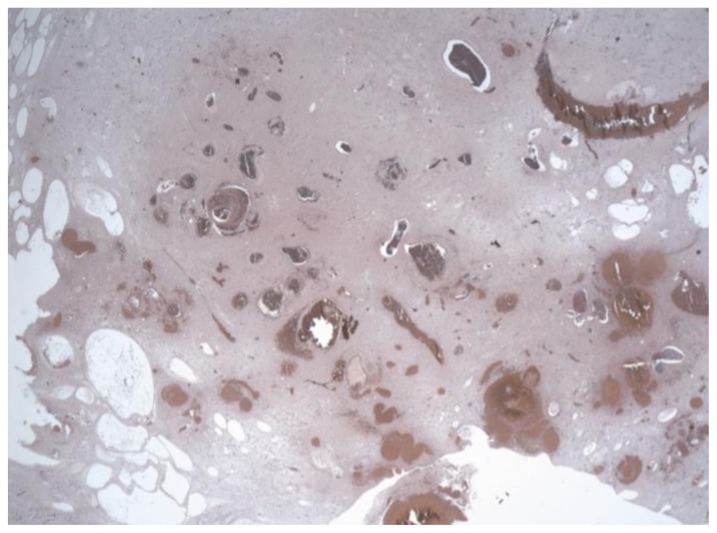
We report a case of a large, heterogeneously enhancing, pathologically proven, supratentorial subependymoma in a 31-year-old male patient presenting with headache, nausea and vomiting as well as gait disturbances. Although most supratentorial subependymomas have distinctive MR features, our case demonstrated imaging findings that made it indistinguishable from other more aggressive malignant supratentorial intraventricular lesions. It is of paramount importance to consider supratentorial subependymomas in the differential diagnosis of supratentorial lesions, even if their radiological features were atypical.
Keywords: MRI; adult; intraventricular; subependymoma; supratentorial; tumor.
Figures








Similar articles
-
Rapid expansion of a previously asymptomatic subependymoma. Case report.J Neurosurg. 2005 Dec;103(6):1084-7. doi: 10.3171/jns.2005.103.6.1084. J Neurosurg. 2005. PMID: 16381197
-
[Subependymoma of the lateral ventricle. A case report].Rev Neurol. 2013 Mar 16;56(6):332-6. Rev Neurol. 2013. PMID: 23483468 Spanish.
-
MRI of intracranial subependymomas.J Comput Assist Tomogr. 1995 Mar-Apr;19(2):264-7. doi: 10.1097/00004728-199503000-00018. J Comput Assist Tomogr. 1995. PMID: 7890853
-
Subependymoma in the third ventricle in a child.Clin Imaging. 2004 Sep-Oct;28(5):381-4. doi: 10.1016/S0899-7071(03)00203-1. Clin Imaging. 2004. PMID: 15471674 Review.
-
Atypical hemorrhagic presentation of a fourth ventricle subependymoma: case report.Neurol Med Chir (Tokyo). 2013;53(11):828-31. doi: 10.2176/nmc.cr2012-0292. Epub 2013 Oct 21. Neurol Med Chir (Tokyo). 2013. PMID: 24140775 Free PMC article. Review.
Cited by
-
A case of septum pellucidum subependymoma with a subtle imaging appearance simulating a cavum septum pellucidum.J Radiol Case Rep. 2013 Oct 1;7(10):7-16. doi: 10.3941/jrcr.v7i10.1561. eCollection 2013 Oct. J Radiol Case Rep. 2013. PMID: 24421918 Free PMC article.
-
Intraventricular Subependymoma With Obstructive Hydrocephalus: A Case Report and Literature Review.Cureus. 2024 Jan 19;16(1):e52563. doi: 10.7759/cureus.52563. eCollection 2024 Jan. Cureus. 2024. PMID: 38371163 Free PMC article.
-
Diagnosis of symmetric bilateral lateral ventricular subependymomas: A case report.Exp Ther Med. 2022 Jun 8;24(2):503. doi: 10.3892/etm.2022.11429. eCollection 2022 Aug. Exp Ther Med. 2022. PMID: 35837028 Free PMC article.
References
-
- Matsumura A, Ahyai A, Hori A, Schaake T. Intracerebral subependymomas: clinical and neuropathological analyses with special reference to the possible existence of a less benign variant. Acta Neurochir (Wien) 1989;(1–2):96. 15–25. - PubMed
-
- Jooma R, Torrens MJ, Bradshaw J, Brownell B. Subependymomas of the forth ventricle: surgical treatment in 12 cases. J Neurosurg. 1985 Apr;62(4):508–512. - PubMed
-
- Lombardi D, Scheithauer BW, Meyer FB, et al. Symptomatic subependymoma: a clinicopathological and flowcytometric study. J Neurosurg. 1991 Oct;75(4):583–588. - PubMed
-
- Scheithauer BW. Symptomatic subependymoma: report of 21 cases with review of the literature. J Neurosurg. 1978 Nov;49(5):689–696. - PubMed
-
- Nishio S, Morioka T, Mihara F, Fikui M. Subependymoma of the lateral ventricles. Neurosurg Rev. 2000 Jun;23(2):98–103. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical