

Presentation of ileal Burkitt lymphoma in children
- PMID: 23365715
- PMCID: PMC3558269
- DOI: 10.3941/jrcr.v6i8.1052
Presentation of ileal Burkitt lymphoma in children
Abstract
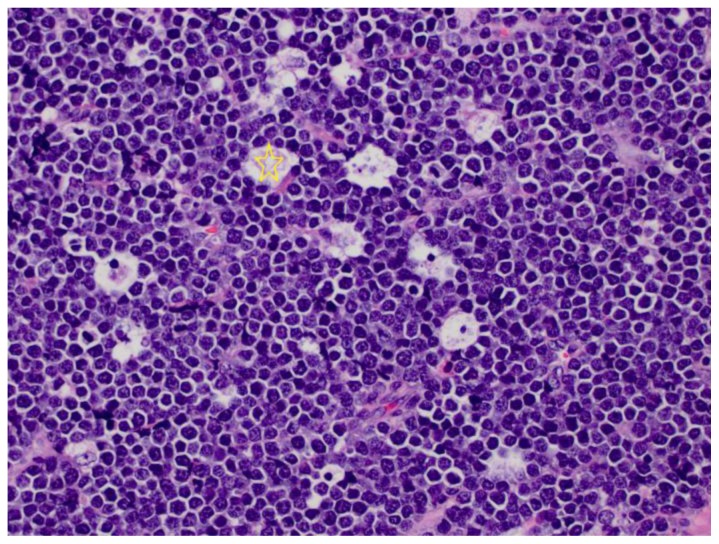
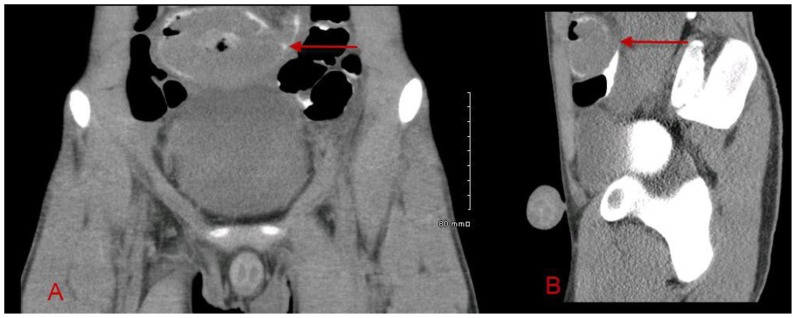
Burkitt lymphoma is a highly aggressive form of Non-Hodgkin lymphoma that responds favorably if diagnosed accurately and treated early. Recognition of the various radiologic manifestations of Burkitt lymphoma can help guide the clinician to expedite appropriate chemotherapy. We present two cases that illustrate different radiologic presentations of this aggressive gastrointestinal malignancy in children. Case 1 features a 7-year-old boy who presented to our hospital with recurrent ileocecal intussusception. Case 2 describes a 16-year-old male with history of blood-streaked stools. Ileocectomy was performed in both cases and histologic analysis showed the "starry sky pattern" and t(8;14) translocation, classic for Burkitt lymphoma. Both patients remain disease-free following surgical excision and chemotherapy.
Keywords: Burkitt; gastrointestinal; lymphoma; pediatric.
Figures












References
-
- Gupta H, Davidoff AM, Pui CH, Shochat SJ, Sandlund JT. Clinical implications and surgical management of intussusception in pediatric patients with Burkitt lymphoma. J Pediatr Surg. 2007;42(6):998–1001. - PubMed
-
- Sorantin E, Lindbichler F. Management of intussusception. Eur Radiol. 2004;14(Suppl 4):L146–154. - PubMed
-
- Kassira N, Pedroso FE, Cheung MC, Koniaris LG, Sola JE. Primary gastrointestinal tract lymphoma in the pediatric patient: review of 265 patients from the SEER registry. J Pediatr Surg. 2011;46:1956–1964. - PubMed
-
- Ferry JA. Burkitt’s lymphoma: clinicopathologic features and differential diagnosis. Oncologist. 2006;11(4):375–383. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical