

Warning for unprincipled colorectal endoscopic submucosal dissection: accurate diagnosis and reasonable treatment strategy
- PMID: 23368854
- PMCID: PMC3615179
- DOI: 10.1111/den.12016
Warning for unprincipled colorectal endoscopic submucosal dissection: accurate diagnosis and reasonable treatment strategy
Abstract
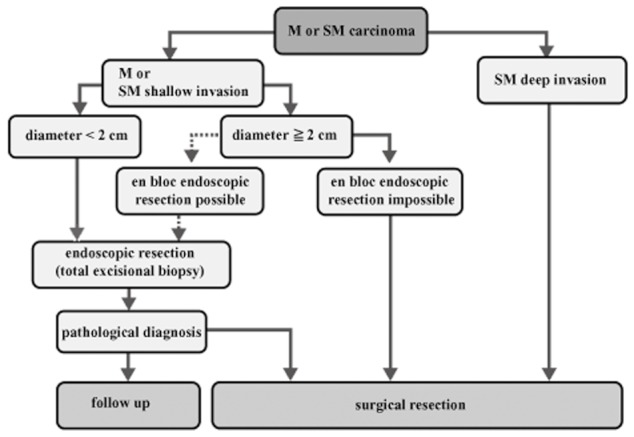
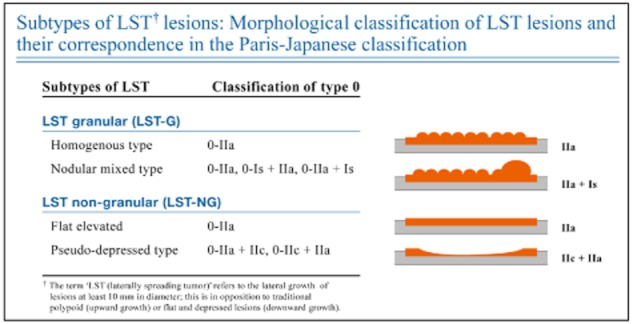
Piecemeal endoscopic mucosal resection (EMR) is generally indicated for laterally spreading tumors (LST) >2 cm in diameter. However, the segmentation of adenomatous parts does not affect the histopathological diagnosis and completeness of cure. Thus, possible indications for piecemeal EMR are both adenomatous homogenous-type granular-type LST (LST-G) and LST-G as carcinoma in adenoma without segmentalizing the carcinomatous part. Diagnosis of the pit pattern using magnifying endoscopy is essential for determining the correct treatment and setting segmentation borders. In contrast, endoscopic submucosal dissection (ESD) is indicated for lesions requiring endoscopic en bloc excision, as it is difficult to use the snare technique for en bloc excisions such as in non-granular-type LST (LST-NG), especially for the pseudodepressed type, tumors with a type VI pit pattern, shallow invasive submucosal carcinoma, largedepressed tumors and large elevated lesions, which are often malignant (e.g. nodular mixed-type LST-G). Other lesions, such as intramucosal tumor accompanied by submucosal fibrosis, induced by biopsy or peristalsis of the lesion; sporadic localized tumors that occur due to chronic inflammation, including ulcerative colitis; and local residual early carcinoma after endoscopic treatment, are also indications for ESD. In clinical practice, an efficient endoscopic treatment with segregation of ESD from piecemeal EMR should be carried out after a comprehensive evaluation of the completeness of cure, safety, clinical simplicity, and cost-benefit, based on an accurate preoperative diagnosis.
© 2012 The Authors. Digestive Endoscopy © 2012 Japan Gastroenterological Endoscopy Society.
Figures
References
-
- Tanaka S, Oka S, Kaneko I, et al. Endoscopic submucosal dissection for colorectal neoplasia: Possibility of standardization. Gastrointest. Endosc. 2007;66:100–107. - PubMed
-
- Tanaka S, Oka S, Chayama K. Colorectal endoscopic submucosal dissection: Present status and future perspective, including its differentiation from endoscopic mucosal resection. J. Gastroenterol. 2008;43:641–651. - PubMed
-
- Gotoda T, Yamamoto H, Soetikno RM. Endoscopic submucosal dissection of early gastric cancer. J. Gastroenterol. 2006;41:929–942. - PubMed
-
- Tanaka S, Terasaki M, Kanao H, Oka S, Chayama K. Current status and future perspectives of endoscopic submucosal dissection for colorectal tumors. Dig. Endosc. 2012;24(Suppl):73–79. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
