

Deep infection in tumor endoprosthesis around the knee: a multi-institutional study by the Japanese musculoskeletal oncology group
- PMID: 23369129
- PMCID: PMC3599741
- DOI: 10.1186/1471-2474-14-51
Deep infection in tumor endoprosthesis around the knee: a multi-institutional study by the Japanese musculoskeletal oncology group
Abstract
Background: The incidence of endoprosthesis failure has been well studied, but few studies have described the clinical characteristics of deep infection in tumor prostheses. This study aimed to analyze the characteristics of deep infection in tumor endoprostheses around the knee.
Methods: We analyzed clinical data of 57 patients with deep infections involving tumor endoprostheses around the knee enrolled from the Japanese Musculoskeletal Oncology Group. Profile of clinical presentation including time between surgery and infection, initial symptoms/blood tests and microbial cultures was evaluated. In addition pre-, intra-, and postoperative clinical factors influencing clinical presentation and treatment outcomes of infections were analyzed.
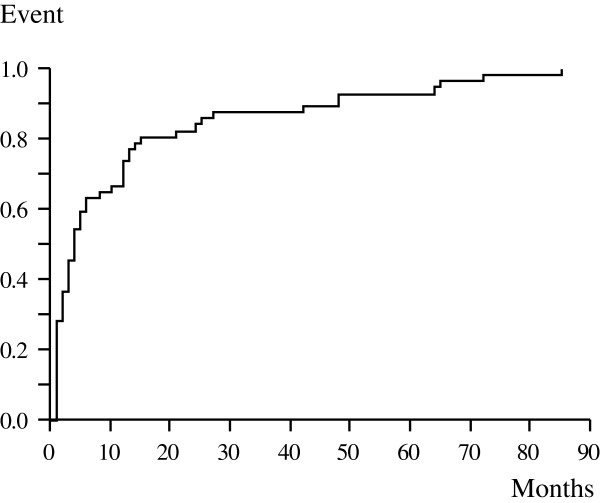
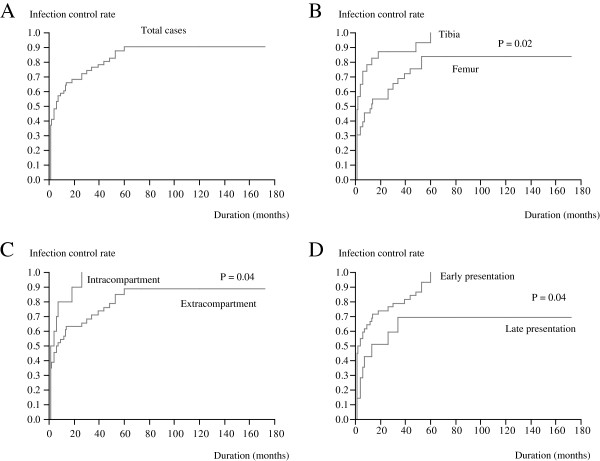
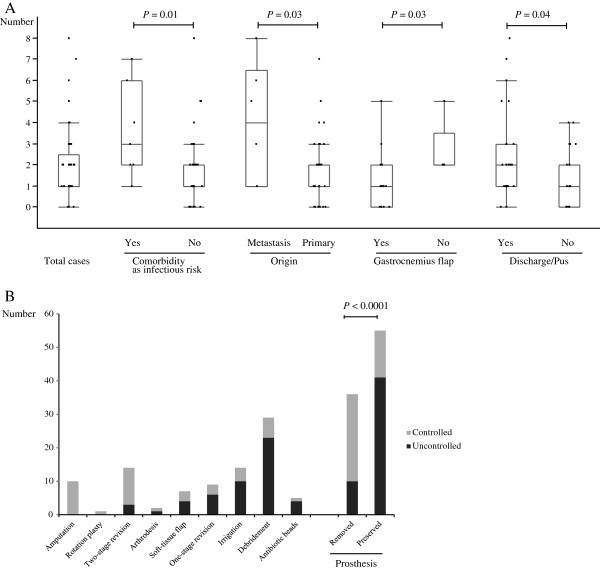
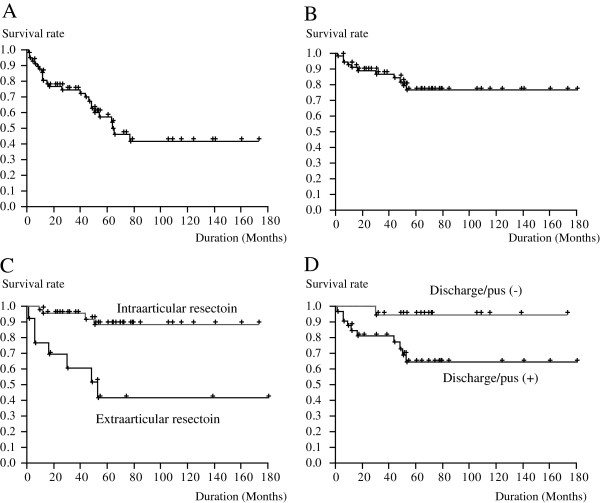
Results: Mean interval between the initial operation and diagnosis was 13 months, and mean time required for infection control was 12 months. The most common pathogen was Staphylococcus. Infection control rates were significantly higher when prostheses were removed rather than salvaged. Ten-year prosthesis survival and limb salvage rates were 41.6% and 75.6%, respectively. Analysis of underlying clinical factors suggested that soft-tissue condition significantly influenced the duration of the infection control period and likelihood of limb salvage.
Conclusions: Infection control is a prolonged process. Deep infection frequently results in amputation or prosthesis loss. Intensive analysis of clinical characteristics may aid infection control.
Figures
References
-
- Henderson ER, Groundland JS, Pala E, Dennis JA, Wooten R, Cheong D, Windhager R, Kotz RI, Mercuri M, Funovics PT, Hornicek FJ, Temple HT, Ruggieri P, Letson GD. Failure mode classification for tumor endoprostheses: retrospective review of five institutions and a literature review. J Bone Joint Surg Am. 2011;93:418–429. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
