

Gastrointestinal symptoms during the first week of intensive care are associated with poor outcome: a prospective multicentre study
- PMID: 23370829
- PMCID: PMC3625421
- DOI: 10.1007/s00134-013-2831-1
Gastrointestinal symptoms during the first week of intensive care are associated with poor outcome: a prospective multicentre study
Abstract
Purpose: The study aimed to develop a gastrointestinal (GI) dysfunction score predicting 28-day mortality for adult patients needing mechanical ventilation (MV).
Methods: 377 adult patients from 40 ICUs with expected duration of MV for at least 6 h were prospectively studied. Predefined GI symptoms, intra-abdominal pressures (IAP), feeding details, organ dysfunction and treatment were documented on days 1, 2, 4 and 7.
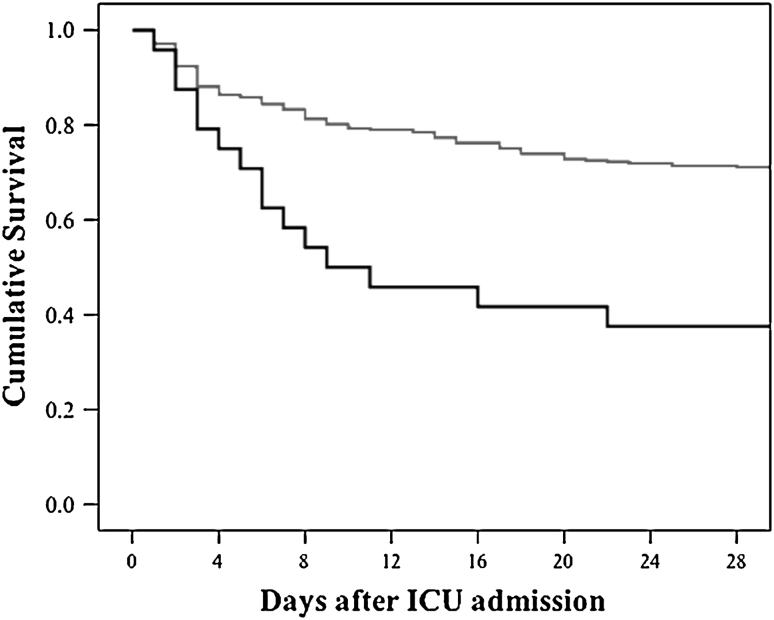
Results: The number of simultaneous GI symptoms was higher in nonsurvivors on each day. Absent bowel sounds and GI bleeding were the symptoms most significantly associated with mortality. None of the GI symptoms alone was an independent predictor of mortality, but gastrointestinal failure (GIF)--defined as three or more GI symptoms--on day 1 in ICU was independently associated with a threefold increased risk of mortality. During the first week in ICU, GIF occurred in 24 patients (6.4%) and was associated with higher 28-day mortality (62.5 vs. 28.9%, P = 0.001). Adding the created subscore for GI dysfunction (based on the number of GI symptoms) to SOFA score did not improve mortality prediction (day 1 AUROC 0.706 [95% CI 0.647-0.766] versus 0.703 [95% CI 0.643-0.762] in SOFA score alone).
Conclusions: An increasing number of GI symptoms independently predicts 28 day mortality with moderate accuracy. However, it was not possible to develop a GI dysfunction score, improving the performance of the SOFA score either due to data set limitations, definition problems, or possibly indicating that GI dysfunction is often secondary and not the primary cause of other organ failure.
Figures

References
-
- Montejo JC. Enteral nutrition-related gastrointestinal complications in critically ill patients: a multicenter study: the Nutritional and Metabolic Working Group of the Spanish Society of Intensive Care Medicine and Coronary Units. Crit Care Med. 1999;27:1447–1453. doi: 10.1097/00003246-199908000-00006. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
