

Corticobasal degeneration with olivopontocerebellar atrophy and TDP-43 pathology: an unusual clinicopathologic variant of CBD
- PMID: 23371366
- PMCID: PMC3633676
- DOI: 10.1007/s00401-013-1087-8
Corticobasal degeneration with olivopontocerebellar atrophy and TDP-43 pathology: an unusual clinicopathologic variant of CBD
Abstract
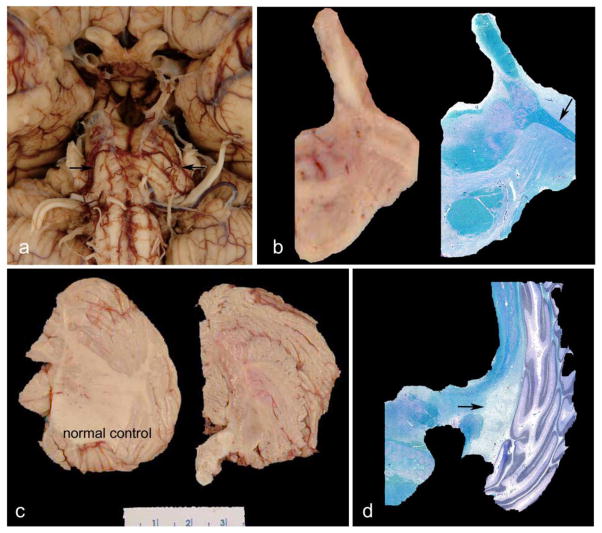
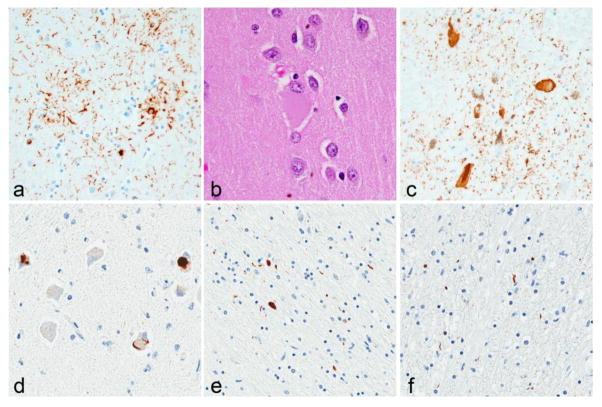
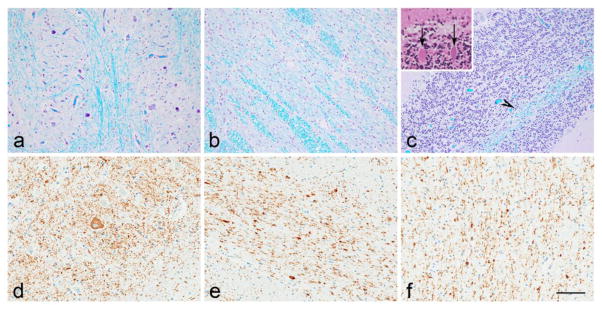
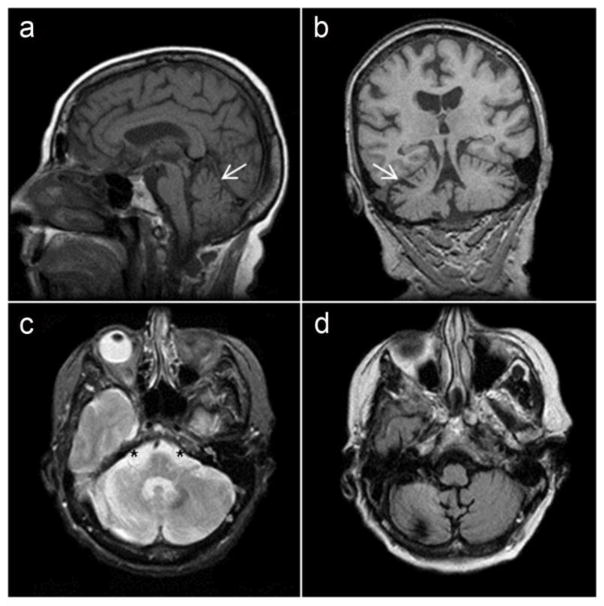
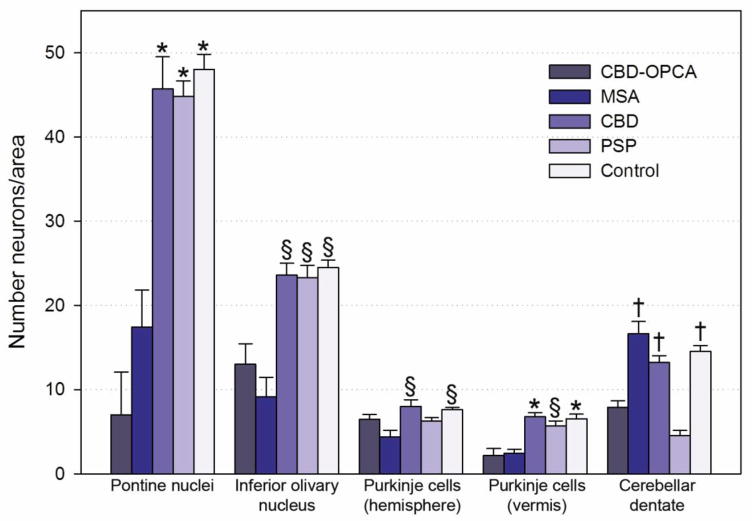
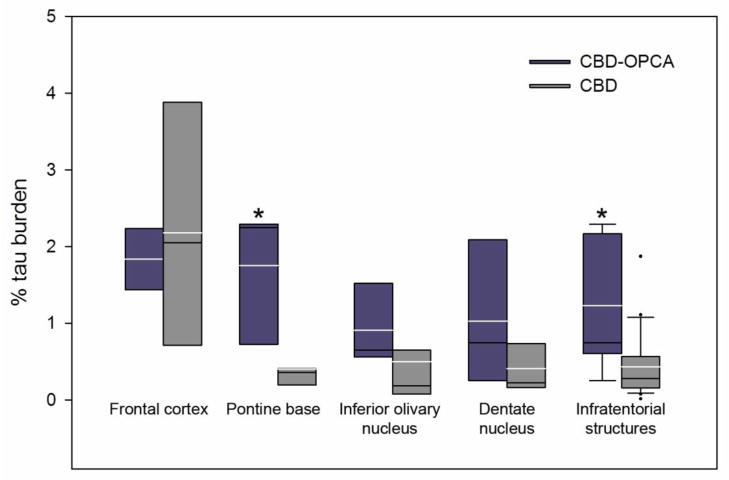
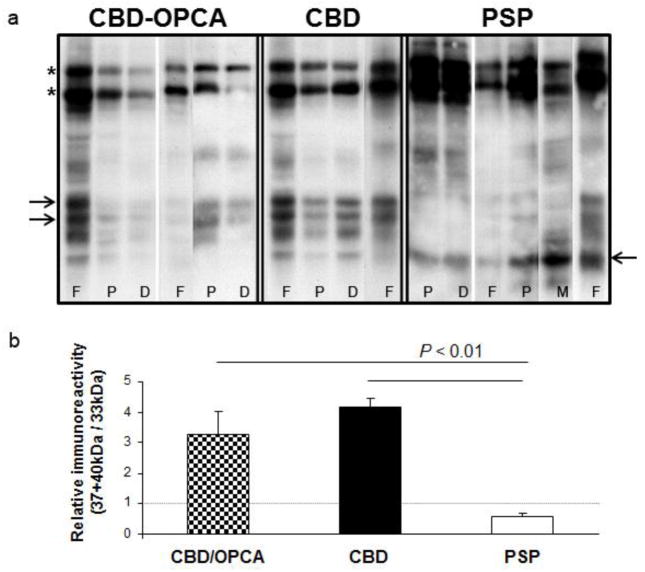
Corticobasal degeneration (CBD) is a disorder affecting cognition and movement due to a progressive neurodegeneration associated with distinctive neuropathologic features, including abnormal phosphorylated tau protein in neurons and glia in cortex, basal ganglia, diencephalon, and brainstem, as well as ballooned neurons and astrocytic plaques. We identified three cases of CBD with olivopontocerebellar atrophy (CBD-OPCA) that did not have α-synuclein-positive glial cytoplasmic inclusions of multiple system atrophy (MSA). Two patients had clinical features suggestive of progressive supranuclear palsy (PSP), and the third case had cerebellar ataxia thought to be due to idiopathic OPCA. Neuropathologic features of CBD-OPCA are compared to typical CBD, as well as MSA and PSP. CBD-OPCA and MSA had marked neuronal loss in pontine nuclei, inferior olivary nucleus, and Purkinje cell layer. Neuronal loss and grumose degeneration in the cerebellar dentate nucleus were comparable in CBD-OPCA and PSP. Image analysis of tau pathology showed greater infratentorial tau burden, especially in pontine base, in CBD-OPCA compared with typical CBD. In addition, CBD-OPCA had TDP-43 immunoreactive neuronal and glial cytoplasmic inclusions and threads throughout the basal ganglia and in olivopontocerebellar system. CBD-OPCA met neuropathologic research diagnostic criteria for CBD and shared tau biochemical characteristics with typical CBD. These results suggest that CBD-OPCA is a distinct clinicopathologic variant of CBD with olivopontocerebellar TDP-43 pathology.
Figures
Similar articles
-
Corticobasal degeneration with TDP-43 pathology presenting with progressive supranuclear palsy syndrome: a distinct clinicopathologic subtype.Acta Neuropathol. 2018 Sep;136(3):389-404. doi: 10.1007/s00401-018-1878-z. Epub 2018 Jun 20. Acta Neuropathol. 2018. PMID: 29926172 Free PMC article.
-
[An autopsied case of progressive supranuclear palsy, initially diagnosed as spinocerebellar degeneration with severe olivopontocerebellar involvement].Rinsho Shinkeigaku. 2011 Oct;51(10):756-60. doi: 10.5692/clinicalneurol.51.756. Rinsho Shinkeigaku. 2011. PMID: 22019867 Japanese.
-
Neuropathologic differentiation of progressive supranuclear palsy and corticobasal degeneration.J Neurol. 1999 Sep;246 Suppl 2:II6-15. doi: 10.1007/BF03161076. J Neurol. 1999. PMID: 10525997 Review.
-
The spectrum of pathological involvement of the striatonigral and olivopontocerebellar systems in multiple system atrophy: clinicopathological correlations.Brain. 2004 Dec;127(Pt 12):2657-71. doi: 10.1093/brain/awh303. Epub 2004 Oct 27. Brain. 2004. PMID: 15509623
-
Astrocytic inclusions in progressive supranuclear palsy and corticobasal degeneration.Neuropathology. 2014 Dec;34(6):555-70. doi: 10.1111/neup.12143. Epub 2014 Aug 14. Neuropathology. 2014. PMID: 25124031 Review.
Cited by
-
Transactivation Response DNA-Binding Protein of 43 (TDP-43) and Glial Cell Roles in Neurological Disorders.Cureus. 2022 Oct 24;14(10):e30639. doi: 10.7759/cureus.30639. eCollection 2022 Oct. Cureus. 2022. PMID: 36439561 Free PMC article. Review.
-
Rapidly Progressive Corticobasal Degeneration Mimicking Brainstem Encephalitis.Mov Disord Clin Pract. 2022 Dec 15;10(2):300-306. doi: 10.1002/mdc3.13633. eCollection 2023 Feb. Mov Disord Clin Pract. 2022. PMID: 36825044 Free PMC article.
-
Distribution and characteristics of transactive response DNA binding protein 43 kDa pathology in progressive supranuclear palsy.Mov Disord. 2017 Feb;32(2):246-255. doi: 10.1002/mds.26809. Epub 2016 Dec 23. Mov Disord. 2017. PMID: 28009087 Free PMC article.
-
Mixed TDP-43 proteinopathy and tauopathy in frontotemporal lobar degeneration: nine case series.J Neurol. 2018 Dec;265(12):2960-2971. doi: 10.1007/s00415-018-9086-2. Epub 2018 Oct 15. J Neurol. 2018. PMID: 30324308 Free PMC article.
-
Neuropathology and pathogenesis of extrapyramidal movement disorders: a critical update-I. Hypokinetic-rigid movement disorders.J Neural Transm (Vienna). 2019 Aug;126(8):933-995. doi: 10.1007/s00702-019-02028-6. Epub 2019 Jun 18. J Neural Transm (Vienna). 2019. PMID: 31214855 Review.
References
-
- Ahmed Z, Doherty KM, Silveira-Moriyama L, et al. Globular glial tauopathies (GGT) presenting with motor neuron disease or frontotemporal dementia: an emerging group of 4-repeat tauopathies. Acta Neuropathol. 2011;122:415–428. - PubMed
-
- Arai T, Ikeda K, Akiyama H, et al. Identification of amino-terminally cleaved tau fragments that distinguish progressive supranuclear palsy from corticobasal degeneration. Ann Neurol. 2004;55:72–79. - PubMed
-
- Arima K, Ueda K, Sunohara N, et al. NACP/alpha-synuclein immunoreactivity in fibrillary components of neuronal and oligodendroglial cytoplasmic inclusions in the pontine nuclei in multiple system atrophy. Acta Neuropathol. 1998;96:439–444. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
