

Sleep disorders and associated medical comorbidities in active duty military personnel
- PMID: 23372263
- PMCID: PMC3543057
- DOI: 10.5665/sleep.2364
Sleep disorders and associated medical comorbidities in active duty military personnel
Abstract
Study objectives: Describe the prevalence of sleep disorders in military personnel referred for polysomnography and identify relationships between demographic characteristics, comorbid diagnoses, and specific sleep disorders.
Design: Retrospective cross-sectional study.
Setting: Military medical treatment facility.
Participants: Active duty military personnel with diagnostic polysomnogram in 2010.
Measurements: Primary sleep disorder rendered by review of polysomnogram and medical record by a board certified sleep medicine physician. Demographic characteristics and conditions of posttraumatic stress disorder (PTSD), mild traumatic brain injury (mTBI), anxiety, depression, and pain syndromes determined by medical record review.
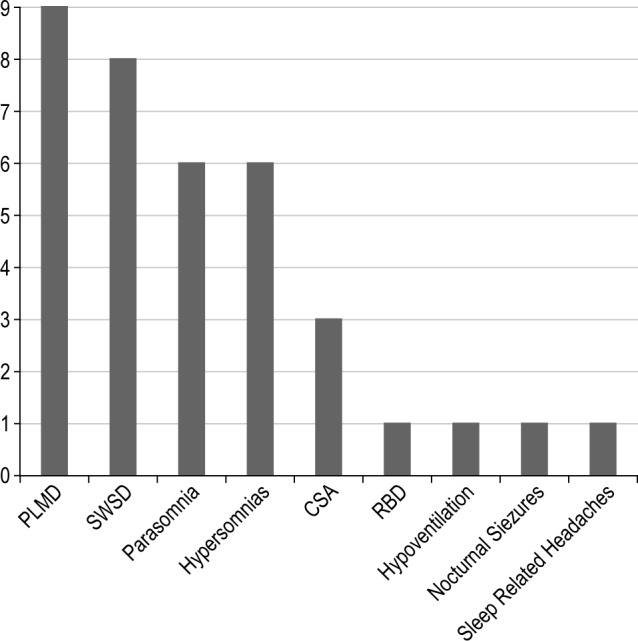
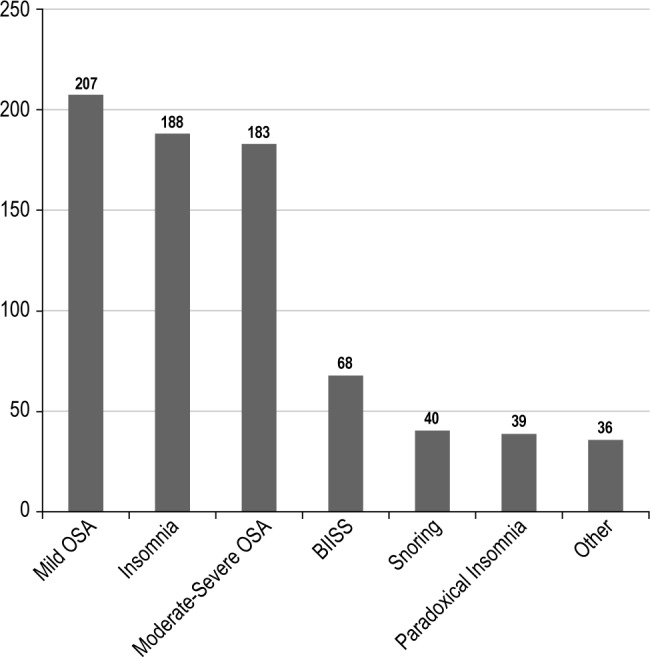
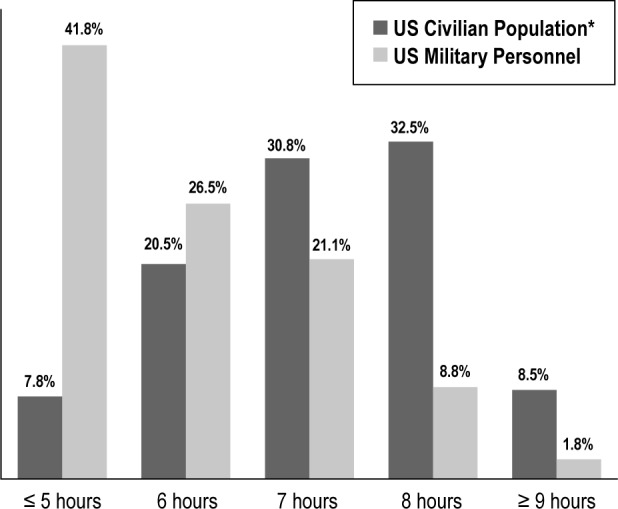
Results: Primary sleep diagnoses (n = 725) included: mild obstructive sleep apnea (OSA), 207 (27.2%); insomnia, 188 (24.7%); moderate-to-severe OSA, 183 (24.0 %); and paradoxical insomnia,39 (5.1%); behaviorally induced insufficient sleep syndrome, 68 (8.9%) and snoring, 40 (5.3%) comprised our control group. Short sleep duration (< 5 h) was reported by 41.8%. Overall 85.2% had deployed, with 58.1% having one or more comorbid diagnoses. Characteristics associated with moderate-to-severe OSA were age (adjusted odds ratio [OR], 1.03 [95% confidence interval {CI}, 1.0-1.05], sex (male) (adjusted OR, 19.97 [95% CI, 2.66-150.05], anxiety (adjusted OR, 0.58 [95% CI, 0.34-0.99]), and body mass index, BMI (adjusted OR 1.19 [95% CI, 1.13-1.25]; for insomnia, characteristics included PTSD (adjusted OR, 2.12 [95% CI, 1.31-3.44]), pain syndromes (adjusted OR, 1.48 [95%CI, 1.01-2.12]), sex (female) (adjusted OR, 0.22 [95% CI, 0.12-0.41]) and lower BMI (adjusted OR, 0.91 [95% CI, 0.87, 0.95]).
Conclusions: Service-related illnesses are prevalent in military personnel who undergo polysomnography with significant associations between PTSD, pain syndromes, and insomnia. Despite having sleep disorders, almost half reported short sleep duration. Multidisciplinary assessment and treatment of military personnel with sleep disorders and service-related illnesses are required.
Citation: Mysliwiec V; McGraw L; Pierce R; Smith P; Trapp B; Roth BJ. Sleep disorders and associated medical comorbidities in active duty military personnel. SLEEP 2013;36(2):167-174.
Figures
Comment in
-
Wounded in action: what the sleep community can learn from sleep disorders of US military service members.Sleep. 2013 Feb 1;36(2):159-60. doi: 10.5665/sleep.2356. Sleep. 2013. PMID: 23372259 Free PMC article. No abstract available.
References
-
- Strengthening our military families: meeting America's commitment. 2012. [Accessed March 9]. http://www.defense.gov/home/features/2011/0111_initiative/strengthening_....
-
- Associations between repeated deployments to OEF/OIF/OND, October 2001-December 2010, and post-deployment illnesses and injuries, active component, U.S. Armed Forces. MSMR. 2011;18:2–11. - PubMed
-
- Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351:13–22. - PubMed
-
- Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. Soldiers returning from Iraq. N Engl J Med. 2008;358:453–63. - PubMed
-
- Peterson AL, Goodie JL, Satterfield WA, Brim WL. Sleep disturbance during military deployment. Mil Med. 2008;173:230–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
