

Epidemiology of perforated peptic ulcer: age- and gender-adjusted analysis of incidence and mortality
- PMID: 23372356
- PMCID: PMC3554818
- DOI: 10.3748/wjg.v19.i3.347
Epidemiology of perforated peptic ulcer: age- and gender-adjusted analysis of incidence and mortality
Abstract
Aim: To investigate the epidemiological trends in incidence and mortality of perforated peptic ulcer (PPU) in a well-defined Norwegian population.
Methods: A retrospective, population-based, single-center, consecutive cohort study of all patients diagnosed with benign perforated peptic ulcer. Included were both gastric and duodenal ulcer patients admitted to Stavanger University Hospital between January 2001 and December 2010. Ulcers with a malignant neoplasia diagnosis, verified by histology after biopsy or resection, were excluded. Patients were identified from the hospitals administrative electronic database using pertinent ICD-9 and ICD-10 codes (K25.1, K25.2, K25.5, K25.6, K26.1, K26.2, K26.5, K26.6). Additional searches using appropriate codes for relevant laparoscopic and open surgical procedures (e.g., JDA 60, JDA 61, JDH 70 and JDH 71) were performed to enable a complete identification of all patients. Patient demographics, presentation patterns and clinical data were retrieved from hospital records and surgical notes. Crude and adjusted incidence and mortality rates were estimated by using national population demographics data.
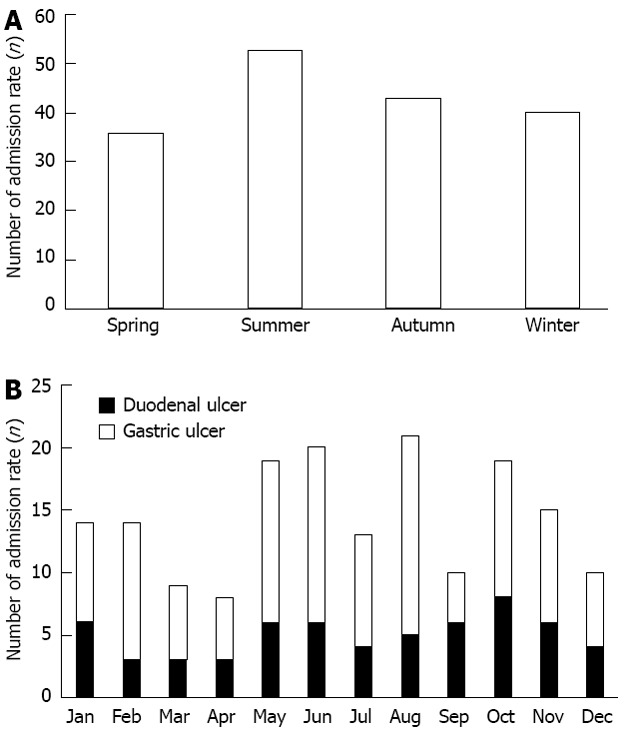
Results: In the study period, a total of 172 patients with PPU were identified. The adjusted incidence rate for the overall 10-year period was 6.5 per 100 000 per year (95%CI: 5.6-7.6) and the adjusted mortality rate for the overall 10-year period was 1.1 per 100 000 per year (95%CI: 0.7-1.6). A non-significant decline in adjusted incidence rate from 9.7 to 5.6 occurred during the decade. The standardized mortality ratio for the whole study period was 5.7 (95%CI: 3.9-8.2), while the total 30-d mortality was 16.3%. No difference in incidence or mortality was found between genders. However, for patients ≥ 60 years, the incidence increased over 10-fold, and mortality more than 50-fold, compared to younger ages. The admission rates outside office hours were high with almost two out of three (63%) admissions seen at evening/night time shifts and/or during weekends. The observed seasonal variations in admissions were not statistically significant.
Conclusion: The adjusted incidence rate, seasonal distribution and mortality rate was stable. PPU frequently presents outside regular work-hours. Increase in incidence and mortality occurs with older age.
Keywords: Epidemiology; Incidence; Mortality; Perforated peptic ulcer; Seasonal variation.
Figures



References
-
- Zelickson MS, Bronder CM, Johnson BL, Camunas JA, Smith DE, Rawlinson D, Von S, Stone HH, Taylor SM. Helicobacter pylori is not the predominant etiology for peptic ulcers requiring operation. Am Surg. 2011;77:1054–1060. - PubMed
-
- Bertleff MJ, Lange JF. Perforated peptic ulcer disease: a review of history and treatment. Dig Surg. 2010;27:161–169. - PubMed
-
- Lau JY, Sung J, Hill C, Henderson C, Howden CW, Metz DC. Systematic review of the epidemiology of complicated peptic ulcer disease: incidence, recurrence, risk factors and mortality. Digestion. 2011;84:102–113. - PubMed
-
- Svanes C. Trends in perforated peptic ulcer: incidence, etiology, treatment, and prognosis. World J Surg. 2000;24:277–283. - PubMed
-
- Møller MH, Adamsen S, Wøjdemann M, Møller AM. Perforated peptic ulcer: how to improve outcome? Scand J Gastroenterol. 2009;44:15–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
